

Subgroup Analysis of Crisaborole for Mild-to-Moderate Atopic Dermatitis in Children Aged 2 to < 18 Years
- PMID: 35292919
- PMCID: PMC8940811
- DOI: 10.1007/s40272-021-00490-y
Subgroup Analysis of Crisaborole for Mild-to-Moderate Atopic Dermatitis in Children Aged 2 to < 18 Years
Abstract
Objectives: This post hoc analysis of pooled data from two phase III studies (AD-301: NCT02118766; AD-302: NCT02118792) explored the efficacy and safety of crisaborole ointment, 2%, a nonsteroidal phosphodiesterase 4 inhibitor, for the treatment of mild-to-moderate atopic dermatitis (AD) in pediatric patients (aged 2 to < 18 years) only, stratified by baseline characteristics.
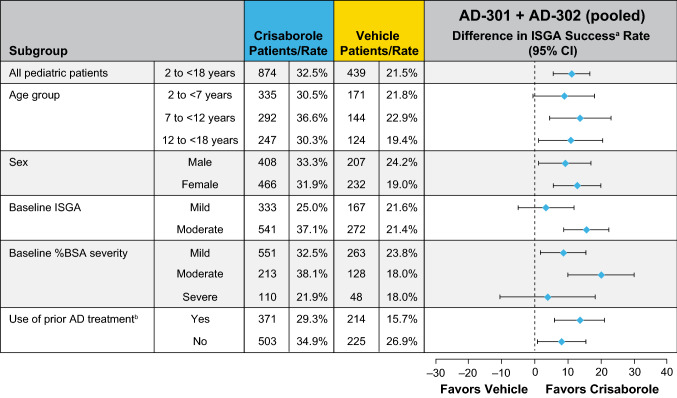
Methods: Pediatric patients with mild or moderate AD per Investigator's Static Global Assessment (ISGA) and percentage of treatable body surface area (%BSA) ≥ 5 at baseline were assessed. Crisaborole or vehicle (2:1 randomization ratio) was applied twice daily for 28 days. Of the 1313 pediatric patients included in this study, 874 received crisaborole and 439 received vehicle. ISGA success was defined as clear (0) or almost clear (1) with ≥ 2-grade improvement from baseline. Efficacy and safety were stratified by age group, sex, baseline ISGA, baseline %BSA per published severity strata, and prior AD therapy.
Results: Overall, the proportions of crisaborole-treated and vehicle-treated pediatric patients with ISGA success at week 4 were 32.5 and 21.5%, respectively. ISGA success rates at day 29 (week 4) were generally higher in crisaborole-treated (21.9-38.1%) than vehicle-treated (15.7-26.9%) patients across subgroups. Rates of treatment-related application site pain were 2.4-10.1% for crisaborole-treated patients and 0.6-2.2% for vehicle-treated patients across subgroups. No new safety concerns were noted in any patient subgroup.
Conclusion: Crisaborole improved global disease severity and was reasonably well tolerated across all pediatric baseline characteristic subgroups. Application site discomfort was greater with crisaborole than with vehicle, but few patients discontinued treatment.
Gov registration numbers: NCT02118766; NCT02118792 (registration date: April 21, 2014).
Plain language summary
Crisaborole is an ointment approved for the treatment of mild-to-moderate eczema. In two phase III clinical trials, eczema improved after 28 days of crisaborole use in patients aged ≥ 2 years. Patients with eczema rashes used crisaborole or plain ointment twice a day for 28 days. The clinical trials excluded patients with serious infections. Eczema treatment within 2 weeks of the trials was not allowed. We looked at whether traits of children aged 2–17 years affected how well crisaborole improved eczema. We studied boys and girls by age and how bad their eczema was at the start of the study. We combined data from both clinical trials to calculate the percentages of children with clear or almost clear skin at day 29. We also studied the frequency of side effects at day 29. After 4 weeks, 33% of children receiving crisaborole compared with 22% of children receiving plain ointment had clear or almost clear skin, a meaningful difference in favor of crisaborole. This was also true across groups. Most patients did not have side effects related to crisaborole. The most common side effect related to crisaborole was application site pain. This side effect occurred in up to one in ten children receiving crisaborole. Up to 1 in 50 patients receiving plain ointment had application site pain. Few children stopped crisaborole treatment, and there were no new safety concerns. In conclusion, compared with plain ointment, crisaborole improved eczema in more children, and side effects were minor.
© 2022. The Author(s).
Conflict of interest statement
Thomas A. Luger has served as an investigator for Pfizer, AbbVie, Celgene, Eli Lilly, LEO Pharma, Menlo Therapeutics, Novartis, and Sandoz; served as a member of scientific advisory boards for Pfizer, AbbVie, Argenx, Celgene, Ceres Pharma, Galderma, Eli Lilly, Janssen-Cilag, La Roche-Posay, LEO Pharma, Menlo Therapeutics, Mylan/Meda AB, Novartis, Pierre Fabre, Piqur Therapeutics, Sandoz, Sanofi-Aventis, and Symrise; and has received funding from Pfizer, AbbVie, Celgene, Janssen-Cilag, Merck Sharp & Dohme, Mylan/Meda AB, Novartis, and Wolff Laboratories. Adelaide A. Hebert discloses that research funding was paid to UTHealth McGovern Medical School from Pfizer, Anacor, Arcutis, Cutanea, Brickell, Dermira, GlaxoSmithKline, and Novan. She has received honoraria as a member of data safety monitoring boards for Bausch, GlaxoSmithKline, and Regeneron-Sanofi and has received honoraria from Pfizer, Biofrontera, Cutanea, Dermavant, Dermira, Galderma, Eli Lilly, Leo Pharma, Ortho Dermatologics, Pierre Fabre, and Verrica. Andrea L. Zaenglein has served as an investigator for AbbVie, Arcutis, Dermavant, Incyte, and Pfizer and as a consultant for Cassiopea and Verrica. Jonathan I. Silverberg has served as an investigator for Celgene, Eli Lilly, F. Hoffmann-La Roche, Menlo Therapeutics, Realm Therapeutics, and Regeneron-Sanofi; as a consultant for Pfizer, AbbVie, Anacor, AnaptysBio, Arena Pharmaceuticals, Dermira, Dermavant, Eli Lilly, Galderma, GlaxoSmithKline, Glenmark, Incyte, Kiniksa, LEO Pharma, Menlo Therapeutics, Novartis, Realm Therapeutics, Regeneron, and Sanofi; and as a speaker for Regeneron and Sanofi. Huaming Tan and Michael A. Zielinski are employees of and stockholders in Pfizer Inc. William C. Ports was an employee of and stockholder in Pfizer Inc. at the time of this analysis.
Figures


References
-
- Bieber T. Atopic dermatitis 2.0: from the clinical phenotype to the molecular taxonomy and stratified medicine. Allergy. 2012;67(12):1475–1482. - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
