

Outcomes in heart failure patients discharged to skilled nursing facilities with delirium
- PMID: 35293145
- PMCID: PMC9065834
- DOI: 10.1002/ehf2.13895
Outcomes in heart failure patients discharged to skilled nursing facilities with delirium
Abstract
Aim: Heart failure (HF) outcomes are disproportionately worse in patients discharged to skilled nursing facilities (SNF) as opposed to home. We hypothesized that dementia and delirium were key factors influencing these differences. Our aim was to explore the associations of dementia and delirium with risk of hospital readmission and mortality in HF patients discharged to SNF.
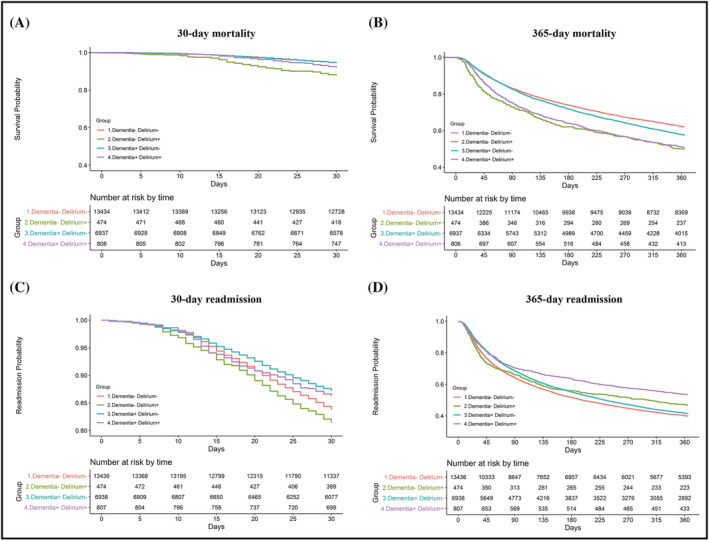
Methods and results: The study population included Veterans hospitalized for a primary diagnosis of HF and discharged to SNFs between 2010 and 2015. Pre-existing dementia was identified based on International Classification of Diseases-9 codes. Delirium was determined using the Minimum Data Set 3.0 Confusion Assessment Method algorithm. Proportional hazard regression analyses were used to model outcomes and were adjusted for covariates of interest. Patients (n = 21 655) were older (77.0 ± 10.5 years) and predominantly male (96.9%). Four groups were created according to presence (+) or absence (-) of dementia and delirium. Relative to the dementia-/delirium- group, the dementia-/delirium+ group was associated with increased 30 day mortality [adjusted hazard ratio (HR) = 2.2, 95% confidence interval (CI) = 1.7, 3.0] and 365 day mortality (adjusted HR = 1.5, 95% CI = 1.3, 1.7). Readmission was highest in the dementia-/delirium+ group after 30 days (HR = 1.2, 95% CI = 1.0, 1.5). In the group with dementia (delirium-/dementia+), 30 day mortality (12.8%; HR = 0.7, 95% CI = 0.7, 0.8) and readmissions (5.3%; HR = 1.0, 95% CI = 0.8, 1.1) were not different relative to the reference group.
Conclusions: Delirium, independent of pre-existing dementia, confers increased risk of hospital readmission and mortality in HF patients discharged to SNFs. Managing HF after hospitalization is a complex cognitive task and an increased focus on mental status in the acute care setting prior to discharge is needed to improve HF management and transitional care, mitigate adverse outcomes, and reduce healthcare costs.
Keywords: Delirium; Dementia; Heart failure; Mortality; Rehabilitation; Skilled nursing facilities.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology. This article has been contributed to by U.S. Government employees and their work is in the public domain in the USA.
Conflict of interest statement
All authors have no relationships with industry to disclose.
Figures
Similar articles
-
Delirium and Functional Recovery in Patients Discharged to Skilled Nursing Facilities After Hospitalization for Heart Failure.JAMA Netw Open. 2021 Mar 1;4(3):e2037968. doi: 10.1001/jamanetworkopen.2020.37968. JAMA Netw Open. 2021. PMID: 33724390 Free PMC article.
-
Association of Positive Delirium Screening with Incident Dementia in Skilled Nursing Facilities.J Am Geriatr Soc. 2020 Dec;68(12):2931-2936. doi: 10.1111/jgs.16830. Epub 2020 Sep 23. J Am Geriatr Soc. 2020. PMID: 32965034 Free PMC article.
-
Risk of Readmission After Discharge From Skilled Nursing Facilities Following Heart Failure Hospitalization: A Retrospective Cohort Study.J Am Med Dir Assoc. 2019 Apr;20(4):432-437. doi: 10.1016/j.jamda.2019.01.135. J Am Med Dir Assoc. 2019. PMID: 30954133 Free PMC article.
-
Heart failure and skilled nursing facilities: review of the literature.J Card Fail. 2012 Nov;18(11):854-71. doi: 10.1016/j.cardfail.2012.09.006. J Card Fail. 2012. PMID: 23141858 Review.
-
Skilled Nursing Facility Care for Patients With Heart Failure: Can We Make It "Heart Failure Ready?".J Card Fail. 2016 Dec;22(12):1004-1014. doi: 10.1016/j.cardfail.2016.10.009. Epub 2016 Oct 18. J Card Fail. 2016. PMID: 27769909 Free PMC article. Review.
Cited by
-
Neuropsychiatric disorders in patients with heart failure: not to be ignored.Heart Fail Rev. 2023 Jul;28(4):821-858. doi: 10.1007/s10741-022-10290-2. Epub 2022 Dec 22. Heart Fail Rev. 2023. PMID: 36547867 Review.
-
Connecting the dots: A narrative review of the relationship between heart failure and cognitive impairment.ESC Heart Fail. 2025 Apr;12(2):1119-1131. doi: 10.1002/ehf2.15144. Epub 2024 Oct 30. ESC Heart Fail. 2025. PMID: 39477682 Free PMC article. Review.
-
Prognostic significance of delirium in patients with heart failure: a systematic review and meta-analysis.Front Cardiovasc Med. 2023 Aug 11;10:1217965. doi: 10.3389/fcvm.2023.1217965. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37636295 Free PMC article. Review.
References
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Piña IL, Trogdon JG, American Heart Association Advocacy Coordinating C , Council on Arteriosclerosis T , Vascular B , Council on Cardiovascular R , Intervention, Council on Clinical C , Council on E, Prevention and Stroke C . Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013; 6: 606–619. - PMC - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després J‐P, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jiménez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER III, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016; 133: e38–e360. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009; 360: 1418–1428. - PubMed
-
- Correale M, Altamura M, Carnevale R, Tricarico L, Malerba S, Gallotta AM, Altamura C, Perrella M, Di Biase M, Bellomo A, Brunetti ND. Delirium in heart failure. Heart Fail Rev. 2020; 25:713–723. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
