

Return to work and sport after a humeral shaft fracture
- PMID: 35293229
- PMCID: PMC8965788
- DOI: 10.1302/2633-1462.33.BJO-2021-0198.R1
Return to work and sport after a humeral shaft fracture
Abstract
Aims: The primary aim of this study was to determine the rates of return to work (RTW) and sport (RTS) following a humeral shaft fracture. The secondary aim was to identify factors independently associated with failure to RTW or RTS.
Methods: From 2008 to 2017, all patients with a humeral diaphyseal fracture were retrospectively identified. Patient demographics and injury characteristics were recorded. Details of pre-injury employment, sporting participation, and levels of return post-injury were obtained via postal questionnaire. The University of California, Los Angeles (UCLA) Activity Scale was used to quantify physical activity among active patients. Regression was used to determine factors independently associated with failure to RTW or RTS.
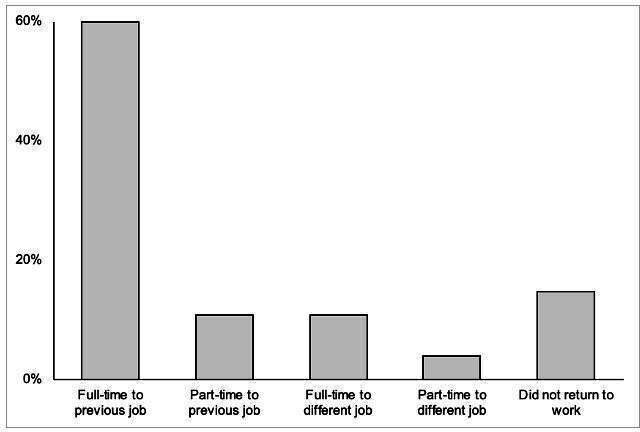
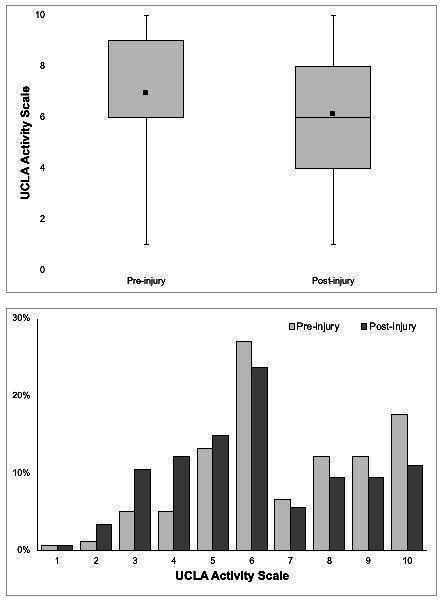
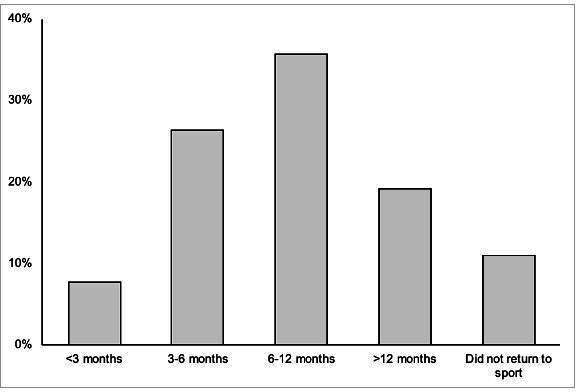
Results: The Work Group comprised 177 patients in employment prior to injury (mean age 47 years (17 to 78); 51% female (n = 90)). Mean follow-up was 5.8 years (1.3 to 11). Overall, 85% (n = 151) returned to work at a mean of 14 weeks post-injury (0 to 104), but only 60% (n = 106) returned full-time to their previous employment. Proximal-third fractures (adjusted odds ratio (aOR) 4.0 (95% confidence interval (CI) 1.2 to 14.2); p = 0.029) were independently associated with failure to RTW. The Sport Group comprised 182 patients involved in sport prior to injury (mean age 52 years (18 to 85); 57% female (n = 104)). Mean follow-up was 5.4 years (1.3 to 11). The mean UCLA score reduced from 6.9 (95% CI 6.6 to 7.2) before injury to 6.1 (95% CI 5.8 to 6.4) post-injury (p < 0.001). There were 89% (n = 162) who returned to sport: 8% (n = 14) within three months, 34% (n = 62) within six months, and 70% (n = 127) within one year. Age ≥ 60 years was independently associated with failure to RTS (aOR 3.0 (95% CI 1.1 to 8.2); p = 0.036). No other factors were independently associated with failure to RTW or RTS.
Conclusion: Most patients successfully return to work and sport following a humeral shaft fracture, albeit at a lower level of physical activity. Patients aged ≥ 60 yrs and those with proximal-third diaphyseal fractures are at increased risk of failing to return to activity. Cite this article: Bone Jt Open 2022;3(3):236-244.
Keywords: Employment; Fischer's exact test; Fracture; Humeral diaphysis; Humeral shaft; Mann-Whitney U test; Nonunion; Orthopaedic Trauma; Physical activity; Sport; Work; chi-squared test; diaphyseal fractures; humeral diaphyseal fractures; humeral shaft fractures; medical comorbidities; nonoperative management.
Figures
References
-
- Oliver WM, Searle HKC, ZH N, Wickramasinghe NRL, Molyneux SG, White TO. Fractures of the proximal- and middle-thirds of the humeral shaft should be considered as fragility fractures: an epidemiological study of 900 consecutive injuries. Bone Joint J. 2020;102-B(11):1475–1483. - PubMed
