

Effect of Early vs Late Supplemental Parenteral Nutrition in Patients Undergoing Abdominal Surgery: A Randomized Clinical Trial
- PMID: 35293973
- PMCID: PMC8928091
- DOI: 10.1001/jamasurg.2022.0269
Effect of Early vs Late Supplemental Parenteral Nutrition in Patients Undergoing Abdominal Surgery: A Randomized Clinical Trial
Abstract
Importance: The effect of and optimal timing for initiating supplemental parenteral nutrition (SPN) remain unclear after major abdominal surgery for patients in whom energy targets cannot be met by enteral nutrition (EN) alone.
Objective: To examine the effect of early supplemental parenteral nutrition (E-SPN) (day 3 after surgery) or late supplemental parenteral nutrition (L-SPN) (day 8 after surgery) on the incidence of nosocomial infections in patients undergoing major abdominal surgery who are at high nutritional risk and have poor tolerance to EN.
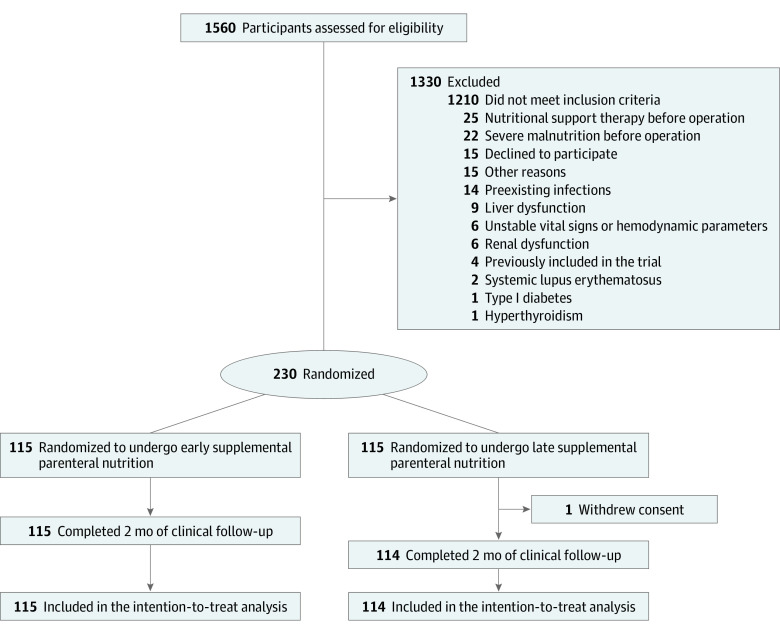
Design, setting, and participants: A multicenter randomized clinical trial was conducted from April 1, 2017, to December 31, 2018, in the general surgery department of 11 tertiary hospitals in China. Participants were those undergoing major abdominal surgery with high nutritional risk and poor tolerance to EN (≤30% of energy targets from EN on postoperative day 2, calculated as 25 and 30 kcal/kg of ideal body weight daily for women and men, respectively) and an expected postoperative hospital stay longer than 7 days. Data analysis was performed from February 1 to October 31, 2020.
Interventions: Random allocation to E-SPN (starting on day 3 after surgery) or L-SPN (starting on day 8 after surgery).
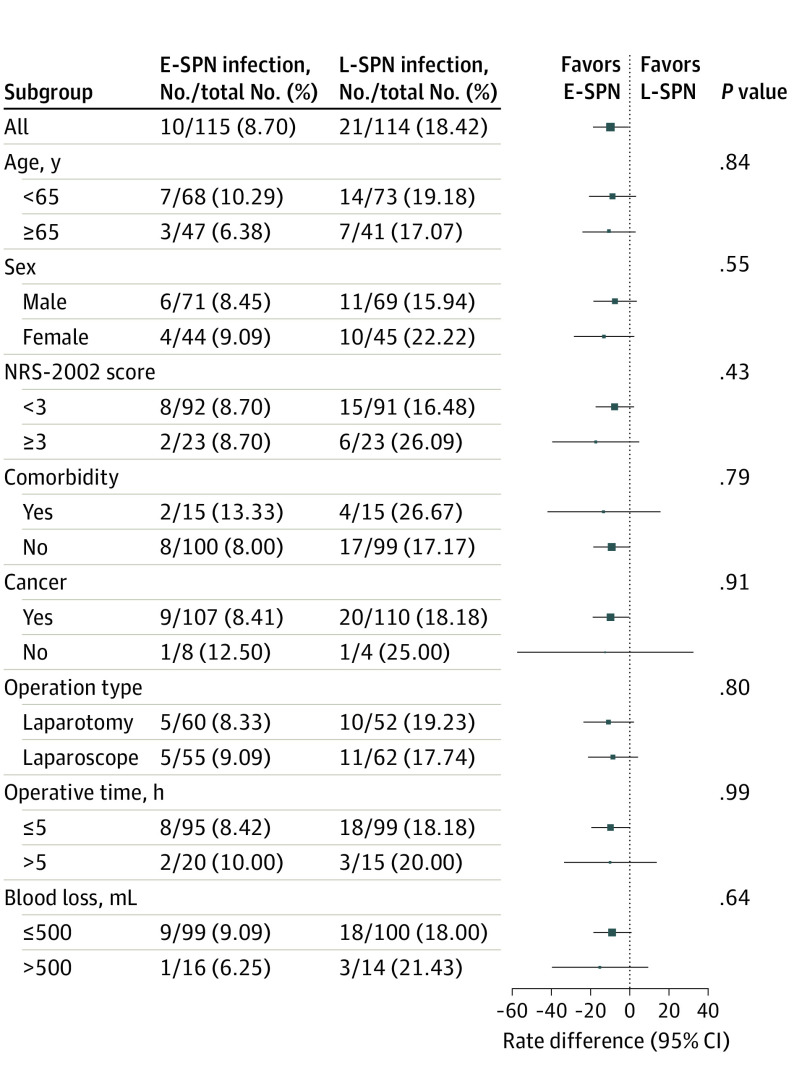
Main outcomes and measures: The primary outcome was the incidence of nosocomial infections between postoperative day 3 and hospital discharge.
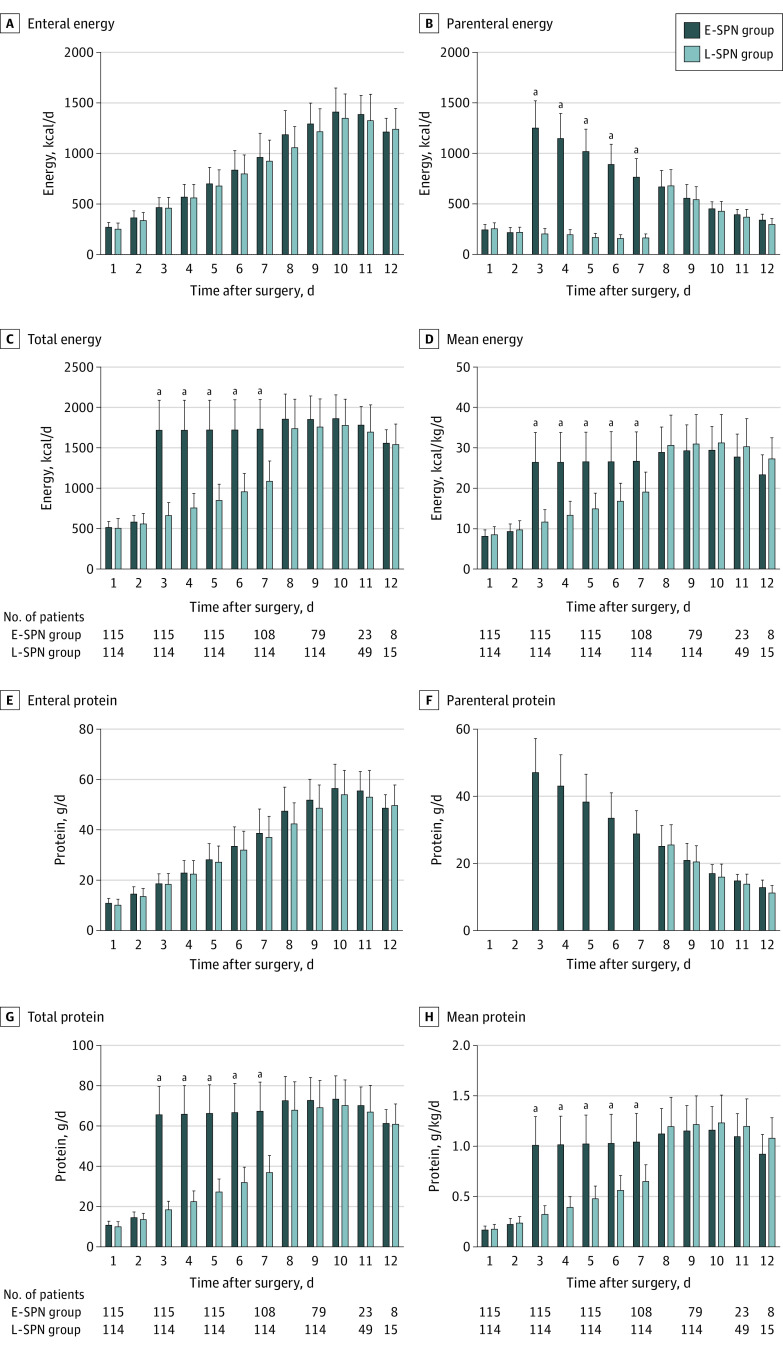
Results: A total of 230 patients (mean [SD] age, 60.1 [11.2] years; 140 men [61.1%]; all patients were of Han race and Asian ethnicity) were randomized (115 to the E-SPN group and 115 to the L-SPN group). One patient in the L-SPN group withdrew informed consent before the intervention. The E-SPN group received more mean (SD) energy delivery between days 3 and 7 compared with the L-SPN group (26.5 [7.4] vs 15.1 [4.8] kcal/kg daily; P < .001). The E-SPN group had significantly fewer nosocomial infections compared with the L-SPN group (10/115 [8.7%] vs 21/114 [18.4%]; risk difference, 9.7%; 95% CI, 0.9%-18.5%; P = .04). No significant differences were found between the E-SPN group and the L-SPN group in the mean (SD) number of noninfectious complications (31/115 [27.0%] vs 38/114 [33.3%]; risk difference, 6.4%; 95% CI, -5.5% to 18.2%; P = .32), total adverse events (75/115 [65.2%] vs 82/114 [71.9%]; risk difference, 6.7%; 95% CI, -5.3% to 18.7%; P = .32), and rates of other secondary outcomes. A significant difference was found in the mean (SD) number of therapeutic antibiotic days between the E-SPN group and the L-SPN group (6.0 [0.8] vs 7.0 [1.1] days; mean difference, 1.0 days; 95% CI, 0.2-1.9 days; P = .01).
Conclusion and relevance: In this randomized clinical trial, E-SPN was associated with reduced nosocomial infections in patients undergoing abdominal surgery and seems to be a favorable strategy for patients with high nutritional risk and poor tolerance to EN after major abdominal surgery.
Trial registration: ClinicalTrials.gov Identifier: NCT03115957.
Conflict of interest statement
Figures
Comment in
-
Early Postoperative Supplementary Parenteral Nutrition.JAMA Surg. 2022 May 1;157(5):393-394. doi: 10.1001/jamasurg.2022.0266. JAMA Surg. 2022. PMID: 35293983 No abstract available.
-
Supplemental Parenteral Nutrition in Patients Undergoing Abdominal Surgery-Reply.JAMA Surg. 2022 Oct 1;157(10):967-968. doi: 10.1001/jamasurg.2022.2655. JAMA Surg. 2022. PMID: 35793111 No abstract available.
-
Supplemental Parenteral Nutrition in Patients Undergoing Abdominal Surgery.JAMA Surg. 2022 Oct 1;157(10):966-967. doi: 10.1001/jamasurg.2022.2654. JAMA Surg. 2022. PMID: 35793119 No abstract available.
-
Supplemental Parenteral Nutrition in Patients Undergoing Abdominal Surgery.JAMA Surg. 2022 Oct 1;157(10):966. doi: 10.1001/jamasurg.2022.2653. JAMA Surg. 2022. PMID: 35793123 No abstract available.
-
JPEN Journal Club 72. The devil in the details.JPEN J Parenter Enteral Nutr. 2023 Mar;47(3):442-444. doi: 10.1002/jpen.2439. Epub 2022 Aug 29. JPEN J Parenter Enteral Nutr. 2023. PMID: 35975333 No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
