

Changes in Triple-Negative Breast Cancer Molecular Subtypes in Patients Without Pathologic Complete Response After Neoadjuvant Systemic Chemotherapy
- PMID: 35294223
- PMCID: PMC8939918
- DOI: 10.1200/PO.20.00368
Changes in Triple-Negative Breast Cancer Molecular Subtypes in Patients Without Pathologic Complete Response After Neoadjuvant Systemic Chemotherapy
Abstract
Purpose: Lehmann et al have identified four molecular subtypes of triple-negative breast cancer (TNBC)-basal-like (BL) 1, BL2, mesenchymal (M), and luminal androgen receptor-and an immunomodulatory (IM) gene expression signature modifier. Our group previously showed that the response of TNBC to neoadjuvant systemic chemotherapy (NST) differs by molecular subtype, but whether NST affects the subtype was unknown. Here, we tested the hypothesis that in patients without pathologic complete response, TNBC subtypes can change after NST. Moreover, in cases with the changed subtype, we determined whether epithelial-to-mesenchymal transition (EMT) had occurred.
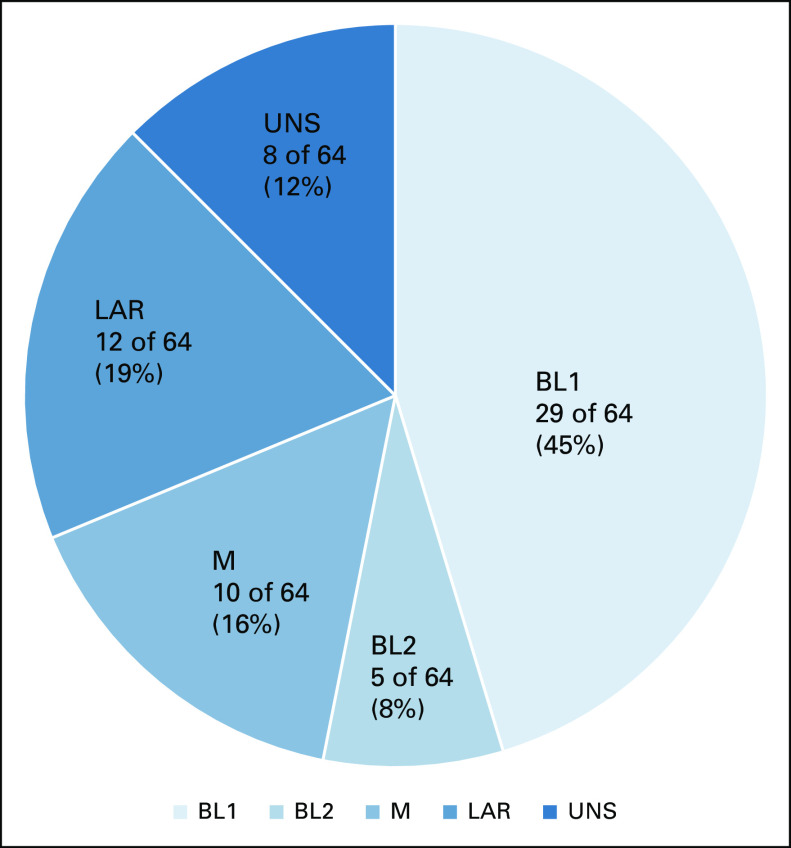
Materials and methods: From the Pan-Pacific TNBC Consortium data set containing TNBC patient samples from four countries, we examined 64 formalin-fixed, paraffin-embedded pairs of matched pre- and post-NST tumor samples. The TNBC subtype was determined using the TNBCtype-IM assay. We analyzed a partial EMT gene expression scoring metric using mRNA data.
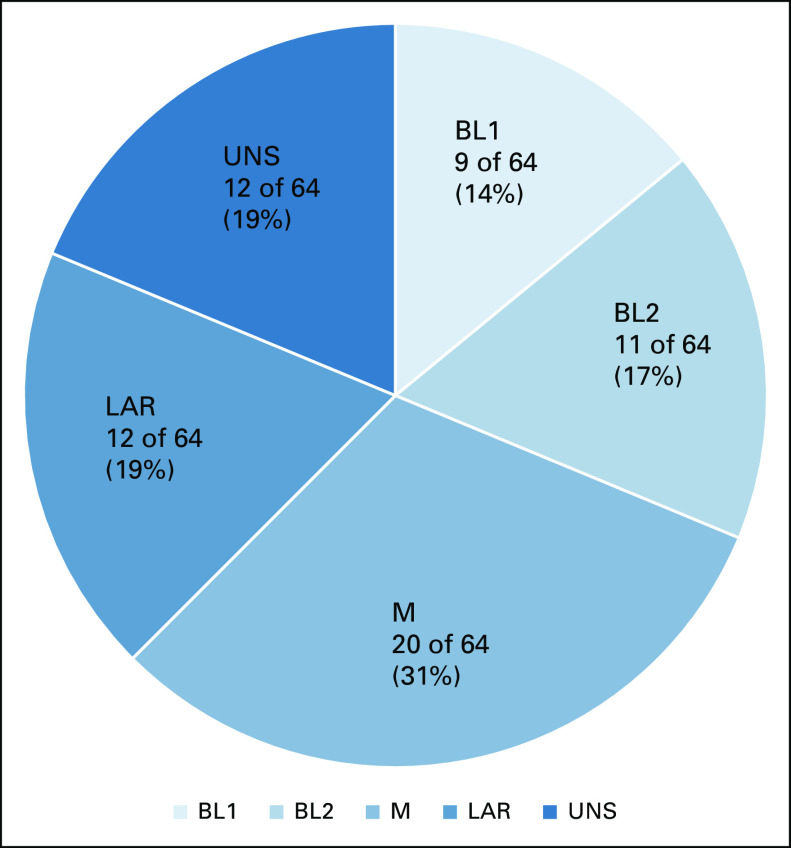
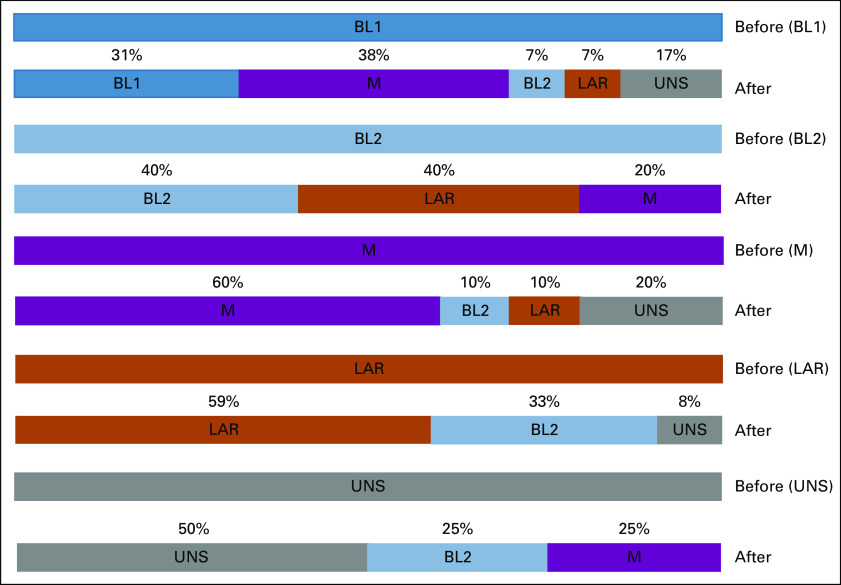
Results: Of the 64 matched pairs, 36 (56%) showed a change in the TNBC subtype after NST. The most frequent change was from BL1 to M subtypes (38%). No tumors changed from M to BL1. The IM signature was positive in 14 (22%) patients before NST and eight (12.5%) patients after NST. The EMT score increased after NST in 28 (78%) of the 36 patients with the changed subtype (v 39% of the 28 patients without change; P = .002254).
Conclusion: We report, to our knowledge, for the first time that the TNBC molecular subtype and IM signature frequently change after NST. Our results also suggest that EMT is promoted by NST. Our findings may lead to innovative adjuvant therapy strategies in TNBC cases with residual tumor after NST.
Conflict of interest statement
Figures
References
-
- Bauer KR, Brown M, Cress RD, et al. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: A population-based study from the California cancer Registry. Cancer. 2007;109:1721–1728. - PubMed
-
- Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin Cancer Res. 2007;13:4429–4434. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
