

Benefit of Continuous Glucose Monitoring in Reducing Hypoglycemia Is Sustained Through 12 Months of Use Among Older Adults with Type 1 Diabetes
- PMID: 35294272
- PMCID: PMC9208859
- DOI: 10.1089/dia.2021.0503
Benefit of Continuous Glucose Monitoring in Reducing Hypoglycemia Is Sustained Through 12 Months of Use Among Older Adults with Type 1 Diabetes
Abstract
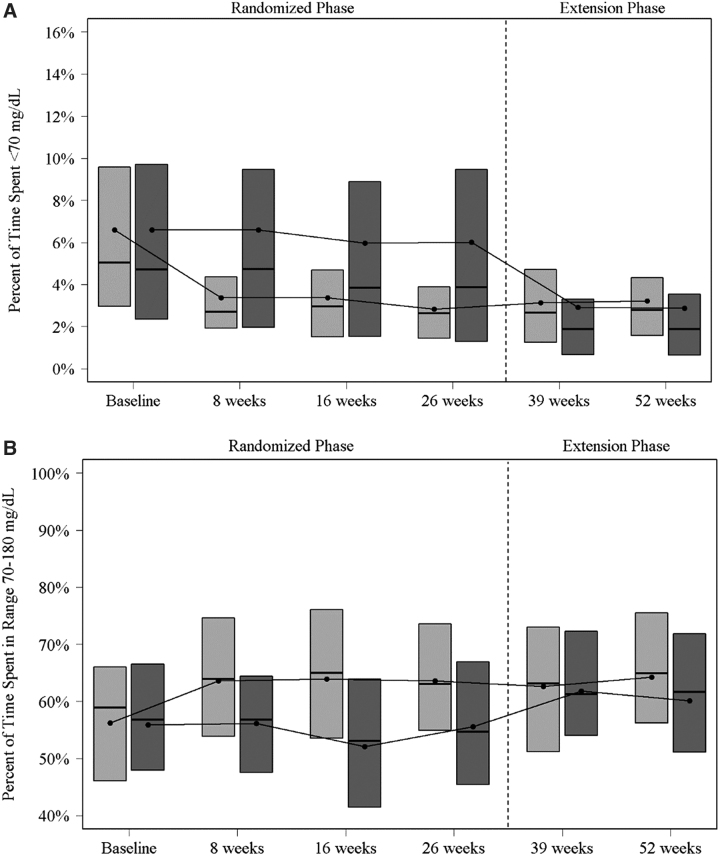
Objective: To evaluate glycemic outcomes in the Wireless Innovation for Seniors with Diabetes Mellitus (WISDM) randomized clinical trial (RCT) participants during an observational extension phase. Research Design and Methods: WISDM RCT was a 26-week RCT comparing continuous glucose monitoring (CGM) with blood glucose monitoring (BGM) in 203 adults aged ≥60 years with type 1 diabetes. Of the 198 participants who completed the RCT, 100 (98%) CGM group participants continued CGM (CGM-CGM cohort) and 94 (98%) BGM group participants initiated CGM (BGM-CGM cohort) for an additional 26 weeks. Results: CGM was used a median of >90% of the time at 52 weeks in both cohorts. In the CGM-CGM cohort, median time <70 mg/dL decreased from 5.0% at baseline to 2.6% at 26 weeks and remained stable with a median of 2.8% at 52 weeks (P < 0.001 baseline to 52 weeks). Participants spent more time in range 70-180 mg/dL (TIR) (mean 56% vs. 64%; P < 0.001) and had lower hemoglobin A1c (HbA1c) (mean 7.6% [59 mmol/mol] vs. 7.4% [57 mmol/mol]; P = 0.01) from baseline to 52 weeks. In BGM-CGM, from 26 to 52 weeks median time <70 mg/dL decreased from 3.9% to 1.9% (P < 0.001), TIR increased from 56% to 60% (P = 0.006) and HbA1c decreased from 7.5% (58 mmol/mol) to 7.3% (57 mmol/mol) (P = 0.025). In BGM-CGM, a severe hypoglycemic event was reported for nine participants while using BGM during the RCT and for two participants during the extension phase with CGM (P = 0.02). Conclusions: CGM use reduced hypoglycemia without increasing hyperglycemia in older adults with type 1 diabetes. These data provide further evidence for fully integrating CGM into clinical practice. Clinicaltrials.gov (NCT03240432).
Keywords: CGM use; Hyperglycemia; Hypoglycemia; Older adults.
Conflict of interest statement
K.M.M. reports nonfinancial support of supplies provided from Dexcom. L.G.K. has nothing to disclose. M.R.R. reports grants from Xeris Pharmaceuticals, personal fees from Semma Therapeutics, and personal fees from Sernova Corporation. A.J.A. reports grants from Dexcom and personal fees from Medtronic. G.A. reports grants from Novo Nordisk, grants from Dexcom, grants from Astra Zeneca, grants from Eli Lilly, grants from Insulet, personal fees from Dexcom, and personal fees from Insulet. LA has nothing to disclose.
A.B. reports grants and other from Sanofi, grants and other from Astra Zeneca, grants and other from Eli Lilly, grants from United BioSource Corporation, grants from Abbott Diabetes Care, grants from Abbvie, grants from Insulet Corporation, grants from Dexcom, grants from Teijin America, Inc., grants from Bayer Healthcare Pharmaceuticals, Inc., grants from Boehringer Ingelheim, grants from Bristol-Meyers Squibb Research and Development, grants from Gan & Lee Pharmaceuticals, grants from JAEB Center for Health Research, grants from KOWA Research Institute, Inc., grants from Medtronic MiniMed, grants from Mylan GmbH, grants from Novo Nordisk, and grants from Theracos Sub LLC outside the submitted work.
B.W.B. reports grants from the employer from Abbott Diabetes Care, Bio-Provention, DexCom, Diasome, Insulet, Janssen, JAEB Center for Health Research, Eli Lilly, Medtronic, Novo Nordisk, Sanvita, Senseonics, Sanofi, Viacyte, and Xeris. B.W.B. has received personal fees for consulting and speaking from Astra Zeneca, Big Foot, Companion Medical, Eli Lilly, MannKind, Medronic, Novo Nordisk, Sanofi, Senseonics, Xeris and Zealand.
A.C. reports grants and other from Novo Nordisk, grants and other from Medtronic, grants and other from Insulet, grants and other from Sanofi, grants from Dexcom, grants and other from Abbott, other from Senseonics, grants and other from Eli Lilly, and grants from UnitedHealth outside the submitted work; in addition, A.C. has a patent to U.S. Provisional Patent Application Serial No. 62/443,004 pending. N.S.C. reports personal fees from Eli Lilly, Inc. G.G. has nothing to disclose. R.G. has nothing to disclose. I.B.H. receives research funding from Medtronic Diabetes, Insulet, and Beta Bionics, and reports consulting from Abbott Diabetes Care and Bigfoot. L.K. reports contract with Lifescan, affiliation with Voluntis. D.K. reports grants and personal fees from Dexcom outside the submitted work. Y.C.K. reports product support from Dexcom and Roche Diabetes and consulting with Novo.
C.J.L. reports grant support from Abbott Diabetes, and grant support and nonfinancial support from Dexcom outside the submitted work, grant support from Insulet, and personal fess from Eli Lilly, Inc. J.B.M. reports personal fees and nonfinancial support from Bayer, personal fees and nonfinancial support from Boehringer Ingelheim, personal fees from Lilly, personal fees from Mannkind, personal fees from Novo Nordisk, personal fees from Salix, and grants and personal fees from Dexcom, grants from Medtronic, grants from NIH, and grants from Leona Helmsley Trust. G.O.M. reports grant support from Abbott Diabetes, and grant support and nonfinancial support from Dexcom outside the submitted work, and grant support from Insulet.
A.P. reports personal fees from Medscape, grants from Dexcom and devices for research received from Abbott Diabetes Care, personal fees from Abbot Diabetes Care, personal fees from MannKind, personal fees from NovoNordisk, personal fees from Eli Lilly, personal fees from Merck, personal fees from Zealand; and Stock options: Omada Health and Teladoc. L.H.P. has nothing to disclose. A.P.T. reports nonfinancial support from Dexcom. R.P.B. reports grants from Dexcom outside the submitted work. M.S. reports personal fees from Lilly. V.N.S. reports receiving research support through University of Colorado from Eli-Lilly, NovoNordisk, Sanofi, Dexcom, vTv therapeutics, Mylan GmbH, and Insulet. V.N.S. also served on advisory board of Sanofi and Medscape LLC. M.J.T. has nothing to disclose. F.V. reports a grant from Tolerion, Inc.
A.V. has nothing to disclose. R.S.W. reports grants from Insulet Corporation, grants from Tolerion, Inc., grants from Eli Lilly and Co, grants from Medtronic, grants from Diasome Pharmaceuticals, and grants from Boehringer Ingelheim. L.A.Y. reports grants from Dexcom, vTv therapeutics, NovoNordisk, Boehringer Ingelheim, Bayer, Sanofi US, Johnson and Johnson, Eli Lilly and Lexicon. R.P. reports grants from Hanmi Pharmaceutical Co.; grants from Janssen; consulting fees from Merck; grants, speaker fees and consulting fees from Novo Nordisk; consulting fees from Pfizer; grants from Poxel SA; grants and consulting fees from Sanofi; consulting fees from Scohia Pharma, Inc.; consulting fees from Sun Pharmaceutical Industries. Fees and honoraria for Dr. Richard Pratley's services were paid for directly to AdventHealth, a nonprofit organization.
Figures
References
-
- The Diabetes Control and Complications Trial Research Group: The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977–986. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
