

Efficacy of Losartan in Hospitalized Patients With COVID-19-Induced Lung Injury: A Randomized Clinical Trial
- PMID: 35294537
- PMCID: PMC8928006
- DOI: 10.1001/jamanetworkopen.2022.2735
Efficacy of Losartan in Hospitalized Patients With COVID-19-Induced Lung Injury: A Randomized Clinical Trial
Erratum in
-
Error in Nonauthor Collaborators.JAMA Netw Open. 2022 May 2;5(5):e2215958. doi: 10.1001/jamanetworkopen.2022.15958. JAMA Netw Open. 2022. PMID: 35579901 Free PMC article. No abstract available.
Abstract
Importance: SARS-CoV-2 viral entry may disrupt angiotensin II (AII) homeostasis, contributing to COVID-19 induced lung injury. AII type 1 receptor blockade mitigates lung injury in preclinical models, although data in humans with COVID-19 remain mixed.
Objective: To test the efficacy of losartan to reduce lung injury in hospitalized patients with COVID-19.
Design, setting, and participants: This blinded, placebo-controlled randomized clinical trial was conducted in 13 hospitals in the United States from April 2020 to February 2021. Hospitalized patients with COVID-19 and a respiratory sequential organ failure assessment score of at least 1 and not already using a renin-angiotensin-aldosterone system (RAAS) inhibitor were eligible for participation. Data were analyzed from April 19 to August 24, 2021.
Interventions: Losartan 50 mg orally twice daily vs equivalent placebo for 10 days or until hospital discharge.
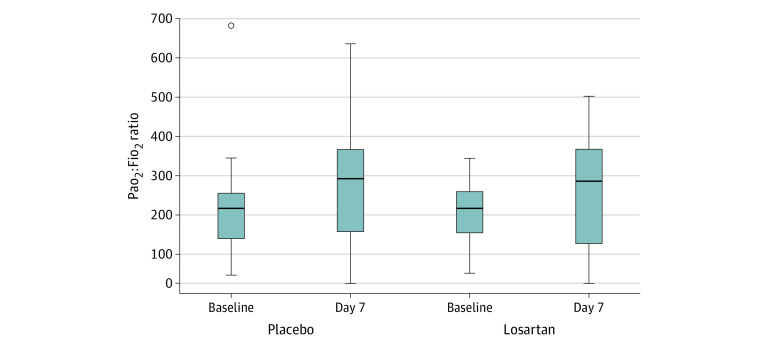
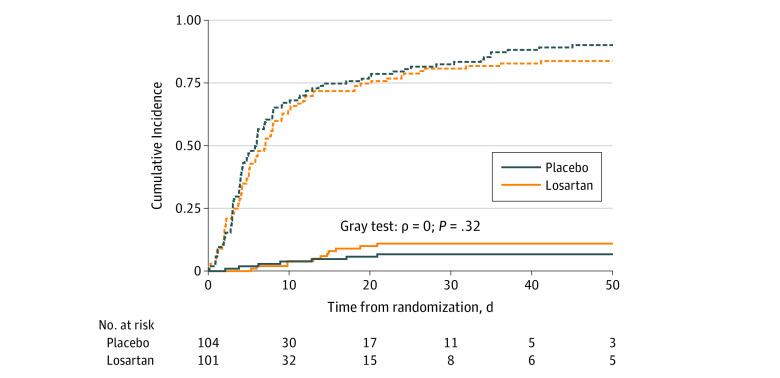
Main outcomes and measures: The primary outcome was the imputed arterial partial pressure of oxygen to fraction of inspired oxygen (Pao2:Fio2) ratio at 7 days. Secondary outcomes included ordinal COVID-19 severity; days without supplemental o2, ventilation, or vasopressors; and mortality. Losartan pharmacokinetics and RAAS components (AII, angiotensin-[1-7] and angiotensin-converting enzymes 1 and 2)] were measured in a subgroup of participants.
Results: A total of 205 participants (mean [SD] age, 55.2 [15.7] years; 123 [60.0%] men) were randomized, with 101 participants assigned to losartan and 104 participants assigned to placebo. Compared with placebo, losartan did not significantly affect Pao2:Fio2 ratio at 7 days (difference, -24.8 [95%, -55.6 to 6.1]; P = .12). Compared with placebo, losartan did not improve any secondary clinical outcomes and led to fewer vasopressor-free days than placebo (median [IQR], 9.4 [9.1-9.8] vasopressor-free days vs 8.7 [8.2-9.3] vasopressor-free days).
Conclusions and relevance: This randomized clinical trial found that initiation of orally administered losartan to hospitalized patients with COVID-19 and acute lung injury did not improve Pao2:Fio2 ratio at 7 days. These data may have implications for ongoing clinical trials.
Trial registration: ClinicalTrials.gov Identifier: NCT04312009.
Conflict of interest statement
Figures

References
-
- Worldometer . COVID-19 coronavirus pandemic. Accessed January 5, 2021. https://www.worldometers.info/coronavirus/
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
