

Assessment of Machine Learning-Based Medical Directives to Expedite Care in Pediatric Emergency Medicine
- PMID: 35294539
- PMCID: PMC8928004
- DOI: 10.1001/jamanetworkopen.2022.2599
Assessment of Machine Learning-Based Medical Directives to Expedite Care in Pediatric Emergency Medicine
Abstract
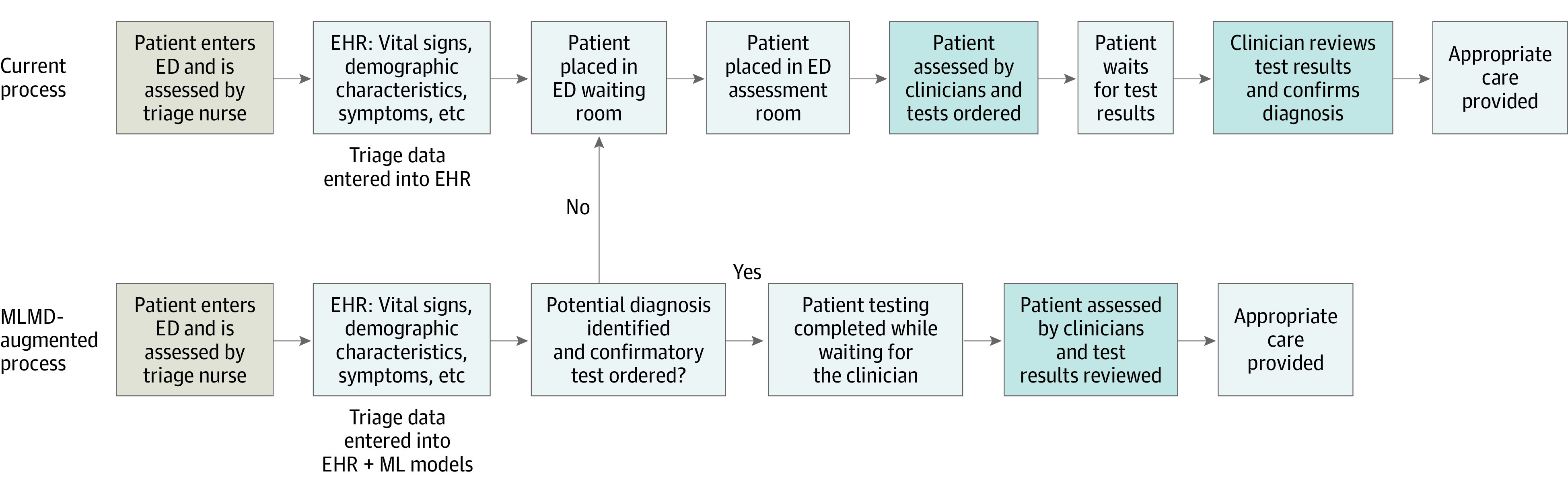
Importance: Increased wait times and long lengths of stay in emergency departments (EDs) are associated with poor patient outcomes. Systems to improve ED efficiency would be useful. Specifically, minimizing the time to diagnosis by developing novel workflows that expedite test ordering can help accelerate clinical decision-making.
Objective: To explore the use of machine learning-based medical directives (MLMDs) to automate diagnostic testing at triage for patients with common pediatric ED diagnoses.
Design, setting, and participants: Machine learning models trained on retrospective electronic health record data were evaluated in a decision analytical model study conducted at the ED of the Hospital for Sick Children Toronto, Canada. Data were collected on all patients aged 0 to 18 years presenting to the ED from July 1, 2018, to June 30, 2019 (77 219 total patient visits).
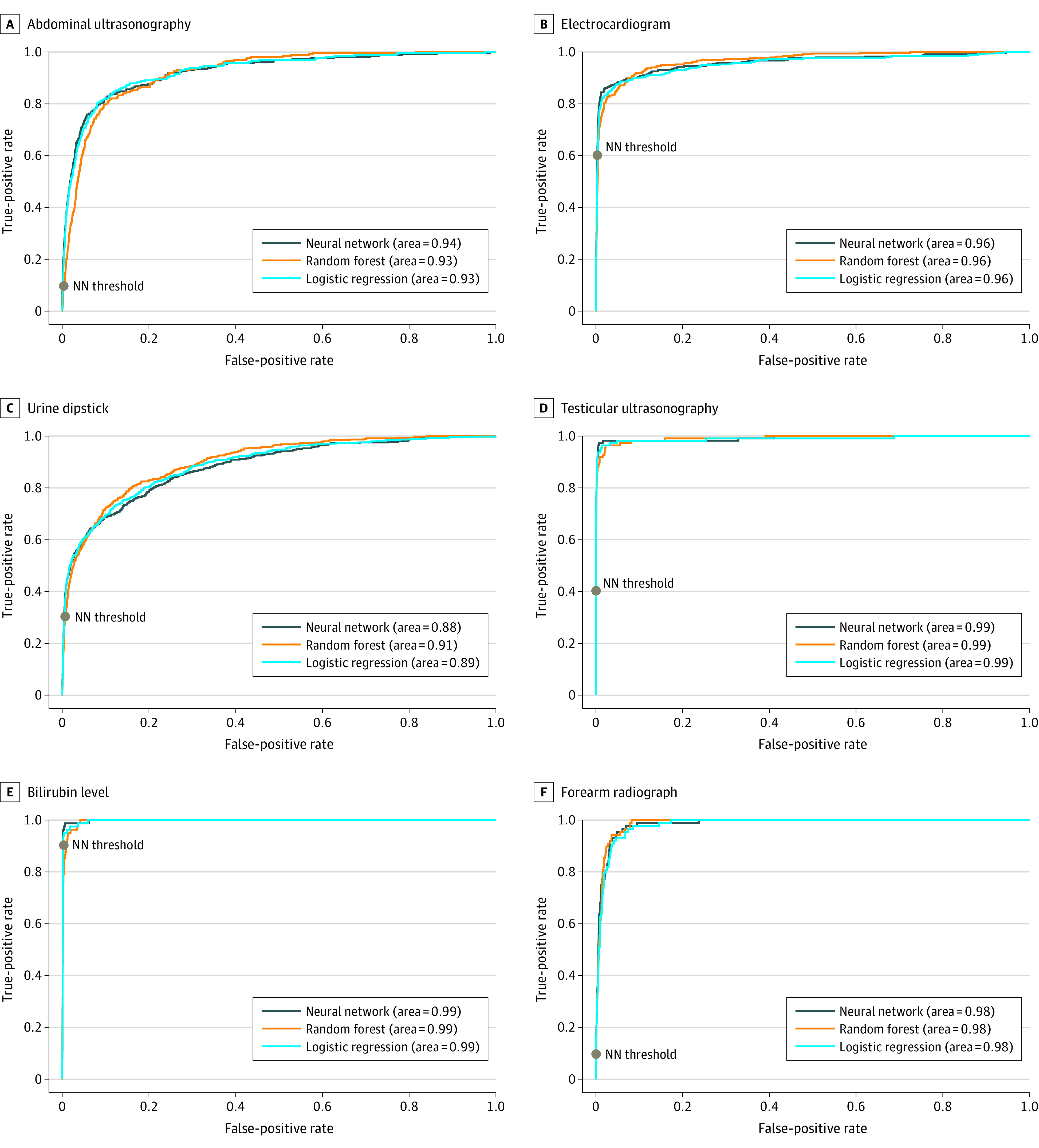
Exposure: Machine learning models were trained to predict the need for urinary dipstick testing, electrocardiogram, abdominal ultrasonography, testicular ultrasonography, bilirubin level testing, and forearm radiographs.
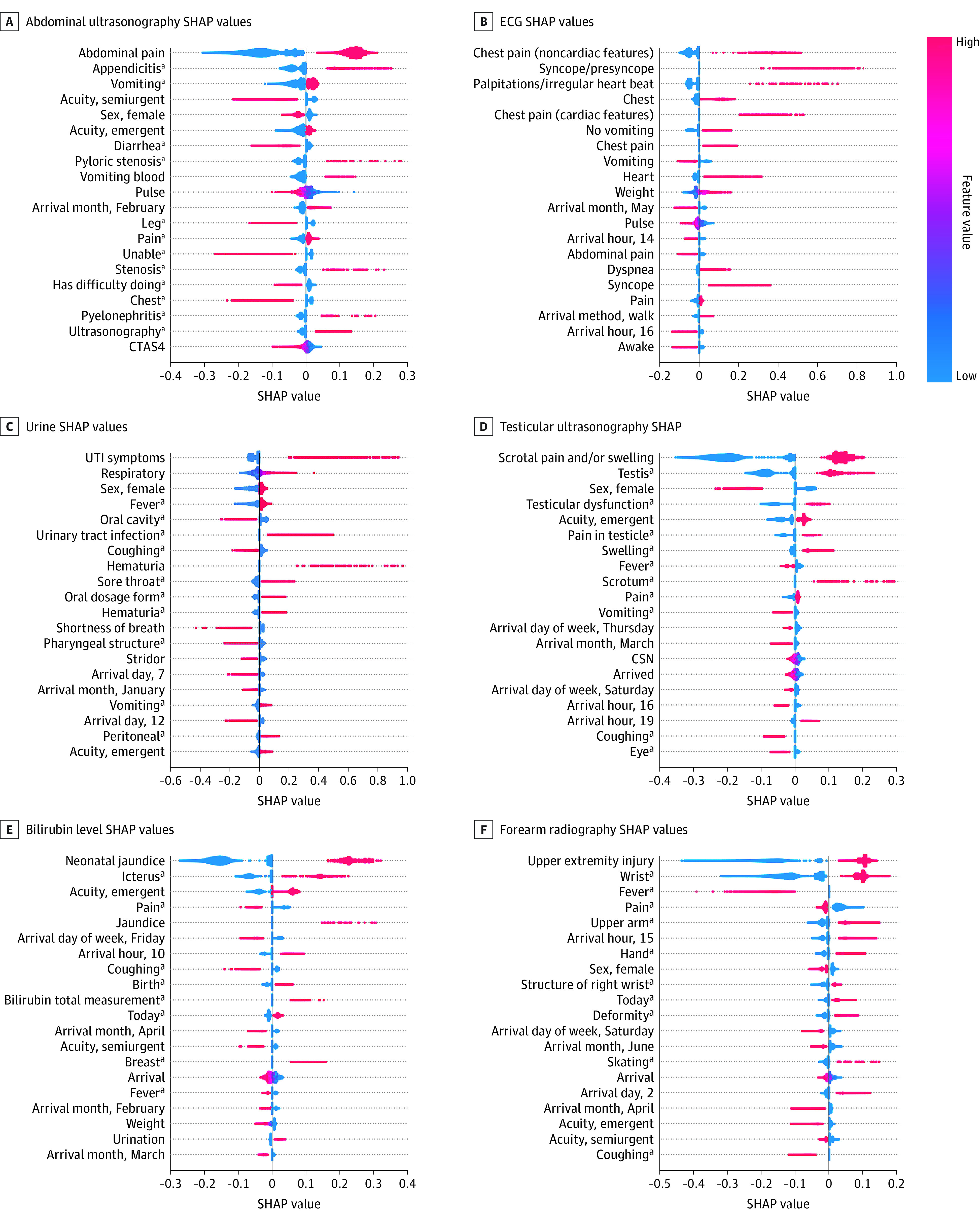
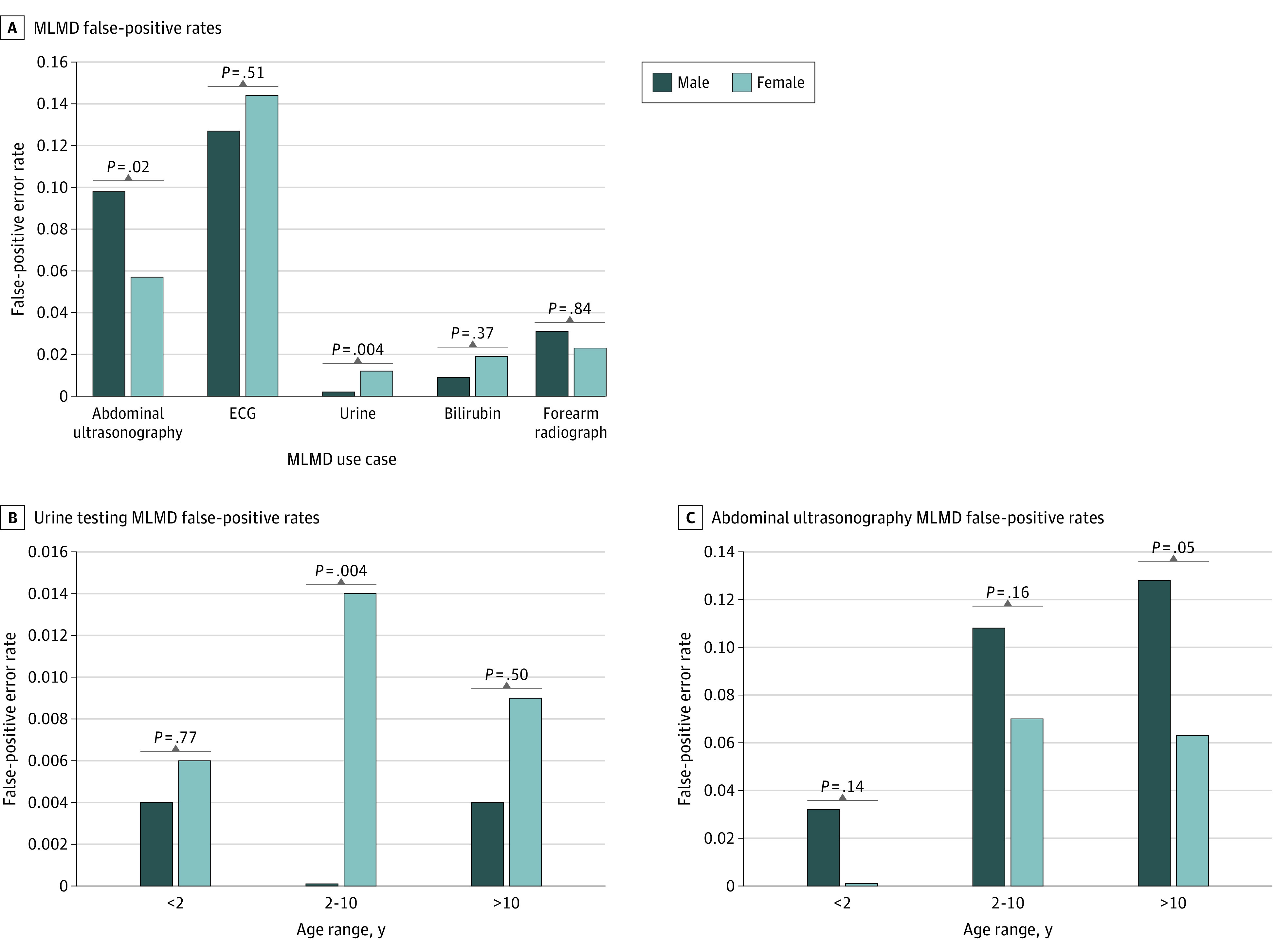
Main outcomes and measures: Models were evaluated using area under the receiver operator curve, true-positive rate, false-positive rate, and positive predictive values. Model decision thresholds were determined to limit the total number of false-positive results and achieve high positive predictive values. The time difference between patient triage completion and test ordering was assessed for each use of MLMD. Error rates were analyzed to assess model bias. In addition, model explainability was determined using Shapley Additive Explanations values.
Results: There was a total of 42 238 boys (54.7%) included in model development; mean (SD) age of the children was 5.4 (4.8) years. Models obtained high area under the receiver operator curve (0.89-0.99) and positive predictive values (0.77-0.94) across each of the use cases. The proposed implementation of MLMDs would streamline care for 22.3% of all patient visits and make test results available earlier by 165 minutes (weighted mean) per affected patient. Model explainability for each MLMD demonstrated clinically relevant features having the most influence on model predictions. Models also performed with minimal to no sex bias.
Conclusions and relevance: The findings of this study suggest the potential for clinical automation using MLMDs. When integrated into clinical workflows, MLMDs may have the potential to autonomously order common ED tests early in a patient's visit with explainability provided to patients and clinicians.
Conflict of interest statement
Figures
Similar articles
-
A Machine Learning Approach to Predicting Need for Hospitalization for Pediatric Asthma Exacerbation at the Time of Emergency Department Triage.Acad Emerg Med. 2018 Dec;25(12):1463-1470. doi: 10.1111/acem.13655. Epub 2018 Nov 29. Acad Emerg Med. 2018. PMID: 30382605
-
Criticality index conducted in pediatric emergency department triage.Am J Emerg Med. 2021 Oct;48:209-217. doi: 10.1016/j.ajem.2021.05.004. Epub 2021 May 6. Am J Emerg Med. 2021. PMID: 33975133
-
Predicting sepsis treatment decisions in the paediatric emergency department using machine learning: the AiSEPTRON study.BMJ Paediatr Open. 2025 May 14;9(1):e003273. doi: 10.1136/bmjpo-2024-003273. BMJ Paediatr Open. 2025. PMID: 40374284 Free PMC article.
-
Machine Learning-Based Prediction of Clinical Outcomes for Children During Emergency Department Triage.JAMA Netw Open. 2019 Jan 4;2(1):e186937. doi: 10.1001/jamanetworkopen.2018.6937. JAMA Netw Open. 2019. PMID: 30646206 Free PMC article.
-
Applications of Artificial Intelligence and Machine Learning in Emergency Medicine Triage - A Systematic Review.Med Arch. 2024;78(3):198-206. doi: 10.5455/medarh.2024.78.198-206. Med Arch. 2024. PMID: 39944197 Free PMC article.
Cited by
-
Teaching old tools new tricks-preparing emergency medicine for the impact of machine learning-based risk prediction models.CJEM. 2023 May;25(5):365-369. doi: 10.1007/s43678-023-00480-8. Epub 2023 Mar 18. CJEM. 2023. PMID: 36933121 Free PMC article. No abstract available.
-
Virtual emergency departments: enabling accessible and compassionate care through inclusive technology.CJEM. 2025 Mar;27(3):157-158. doi: 10.1007/s43678-025-00878-6. CJEM. 2025. PMID: 40067646 No abstract available.
-
Medico-legal risk and use of medical directives in the emergency department.CJEM. 2023 Jul;25(7):589-597. doi: 10.1007/s43678-023-00522-1. Epub 2023 May 12. CJEM. 2023. PMID: 37170059
-
Self-supervised machine learning using adult inpatient data produces effective models for pediatric clinical prediction tasks.J Am Med Inform Assoc. 2023 Nov 17;30(12):2004-2011. doi: 10.1093/jamia/ocad175. J Am Med Inform Assoc. 2023. PMID: 37639620 Free PMC article.
-
A Systematic Integration of Artificial Intelligence Models in Appendicitis Management: A Comprehensive Review.Diagnostics (Basel). 2025 Mar 28;15(7):866. doi: 10.3390/diagnostics15070866. Diagnostics (Basel). 2025. PMID: 40218216 Free PMC article. Review.
