

The role of acute hypercapnia on mortality and short-term physiology in patients mechanically ventilated for ARDS: a systematic review and meta-analysis
- PMID: 35294565
- PMCID: PMC8924945
- DOI: 10.1007/s00134-022-06640-1
The role of acute hypercapnia on mortality and short-term physiology in patients mechanically ventilated for ARDS: a systematic review and meta-analysis
Abstract
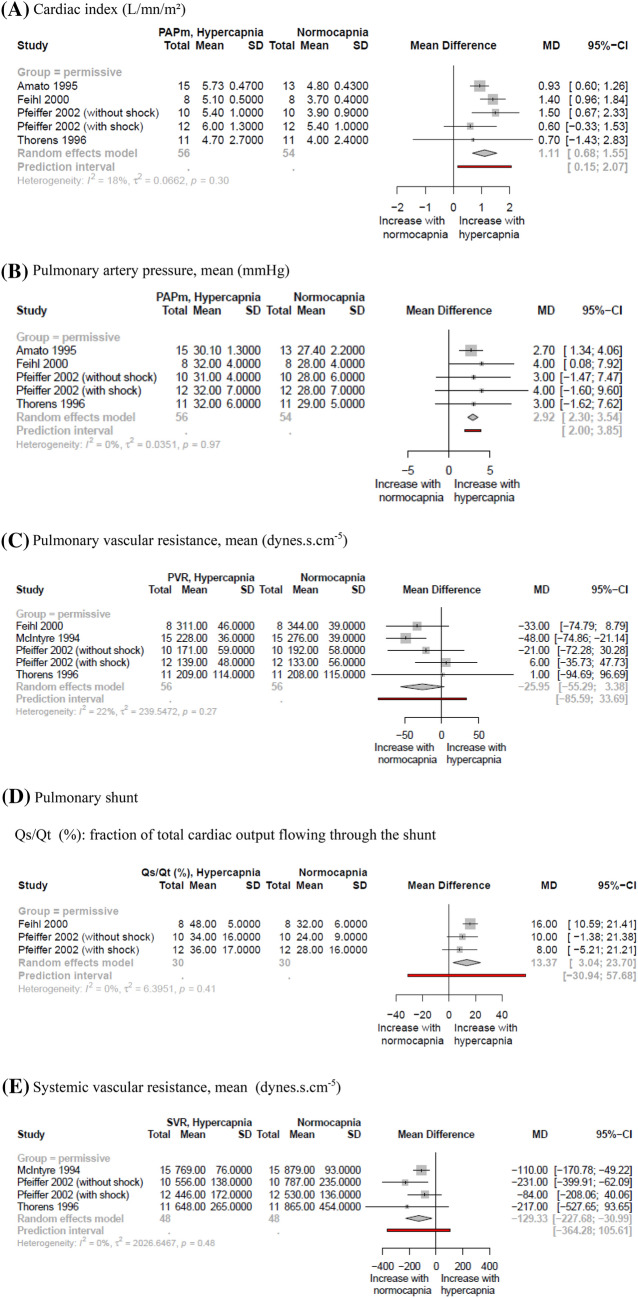
Purpose: Hypercapnia is frequent during mechanical ventilation for acute respiratory distress syndrome (ARDS), but its effects on morbidity and mortality are still controversial. We conducted a systematic review and meta-analysis to explore clinical consequences of acute hypercapnia in adult patients ventilated for ARDS.
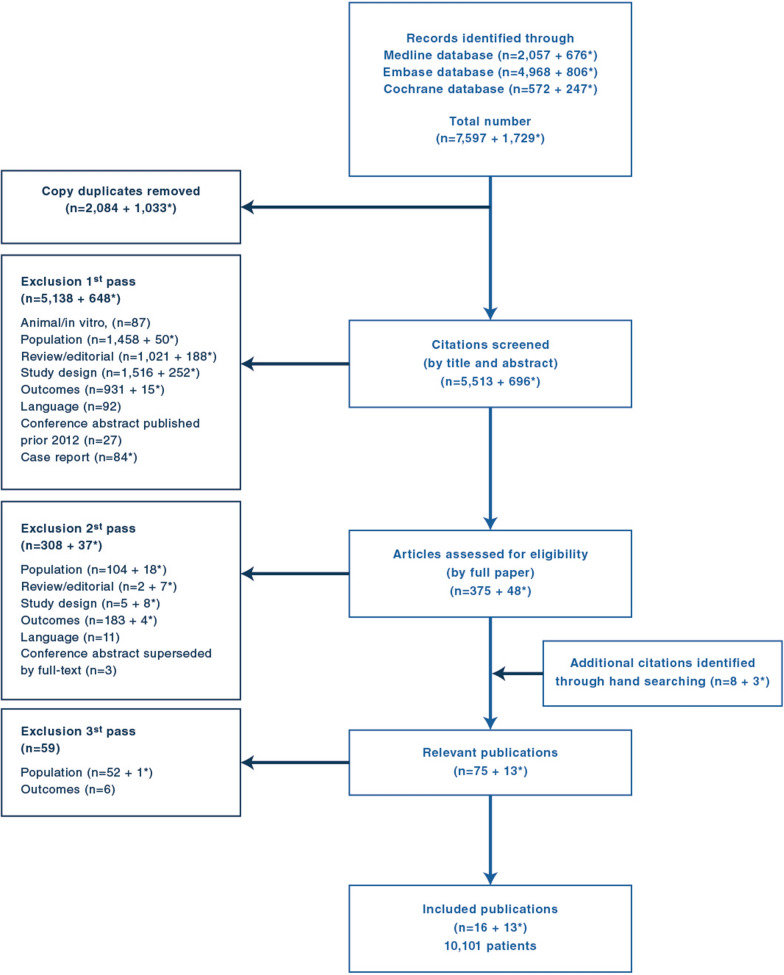
Methods: We searched Medline, Embase, and the Cochrane Library via the OVID platform for studies published from 1946 to 2021. "Permissive hypercapnia" defined hypercapnia in studies where the group with hypercapnia was ventilated with a protective ventilation (PV) strategy (lower VT targeting 6 ml/kg predicted body weight) while the group without hypercapnia was managed with a non-protective ventilation (NPV); "imposed hypercapnia" defined hypercapnia in studies where hypercapnic and non-hypercapnic patients were managed with a similar ventilation strategy.
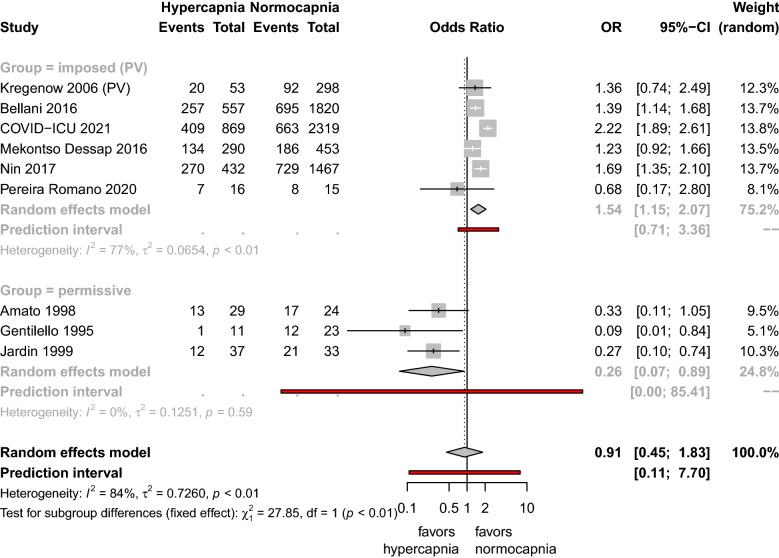
Results: Twenty-nine studies (10,101 patients) were included. Permissive hypercapnia, imposed hypercapnia under PV, and imposed hypercapnia under NPV were reported in 8, 21 and 1 study, respectively. Studies testing permissive hypercapnia reported lower mortality in hypercapnic patients receiving PV as compared to non-hypercapnic patients receiving NPV: OR = 0.26, 95% CI [0.07-0.89]. By contrast, studies reporting imposed hypercapnia under PV reported increased mortality in hypercapnic patients receiving PV as compared to non-hypercapnic patients also receiving PV: OR = 1.54, 95% CI [1.15-2.07]. There was a significant interaction between the mechanism of hypercapnia and the effect on mortality.
Conclusions: Clinical effects of hypercapnia are conflicting depending on its mechanism. Permissive hypercapnia was associated with improved mortality contrary to imposed hypercapnia under PV, suggesting a major role of PV strategy on the outcome.
Keywords: ARDS; Hemodynamics; Hypercapnia.
© 2022. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures

Comment in
-
What about permissive acidosis?Intensive Care Med. 2022 Jun;48(6):785-786. doi: 10.1007/s00134-022-06696-z. Epub 2022 Apr 20. Intensive Care Med. 2022. PMID: 35441850 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
