

Effect of cocoa flavanol supplementation for the prevention of cardiovascular disease events: the COcoa Supplement and Multivitamin Outcomes Study (COSMOS) randomized clinical trial
- PMID: 35294962
- PMCID: PMC9170467
- DOI: 10.1093/ajcn/nqac055
Effect of cocoa flavanol supplementation for the prevention of cardiovascular disease events: the COcoa Supplement and Multivitamin Outcomes Study (COSMOS) randomized clinical trial
Abstract
Background: Cocoa extract is a source of flavanols that favorably influence vascular risk factors in small and short-term trials, yet effects on clinical cardiovascular events are untested.
Objectives: We examined whether cocoa extract supplementation decreases total cardiovascular disease (CVD) among older adults.
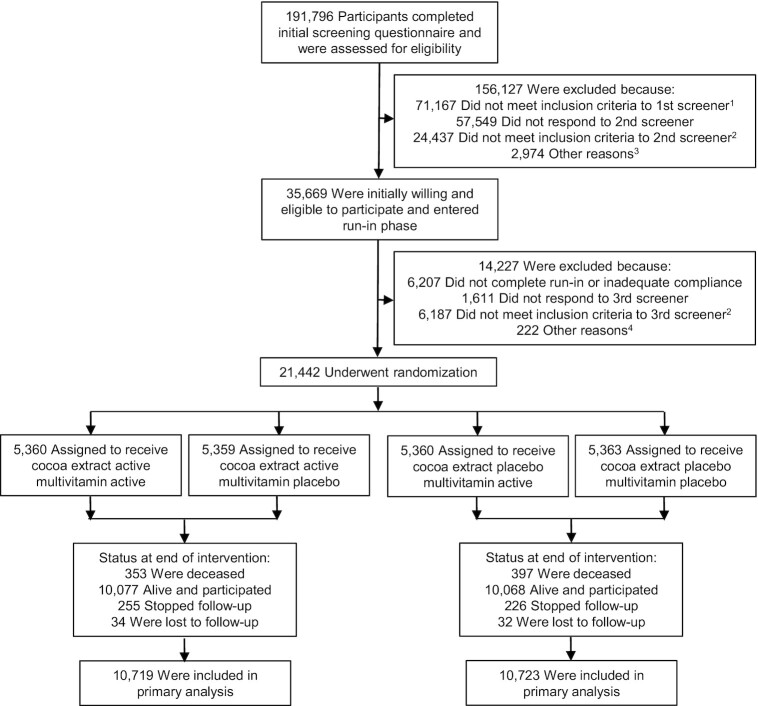
Methods: We conducted a randomized, double-blind, placebo-controlled, 2-by-2 factorial trial of cocoa extract supplementation and multivitamins for prevention of CVD and cancer among 21,442 US adults (12,666 women aged ≥65 y and 8776 men aged ≥60 y), free of major CVD and recently diagnosed cancer. The intervention phase was June 2015 through December 2020. This article reports on the cocoa extract intervention. Participants were randomly assigned to a cocoa extract supplement [500 mg flavanols/d, including 80 mg (-)-epicatechin] or placebo. The primary outcome was a composite of confirmed incident total cardiovascular events, including myocardial infarction (MI), stroke, coronary revascularization, cardiovascular death, carotid artery disease, peripheral artery surgery, and unstable angina.
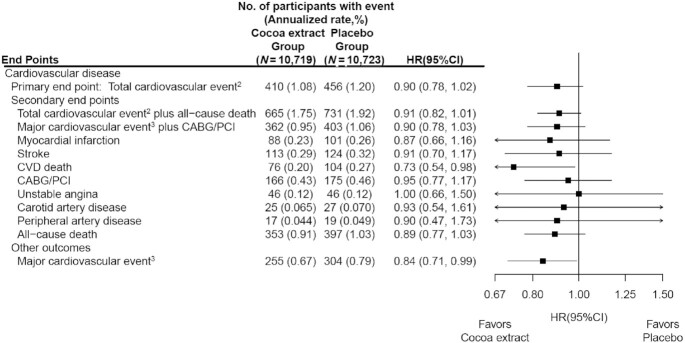
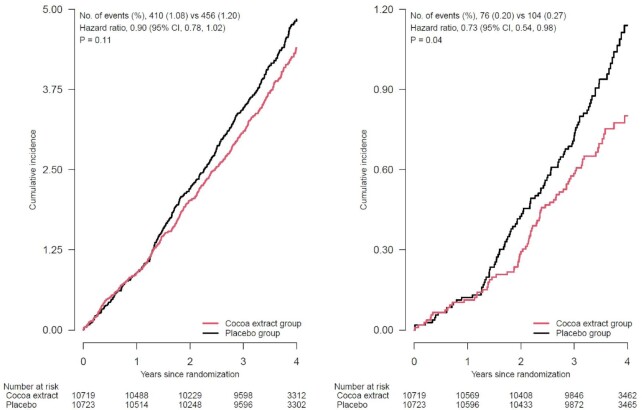
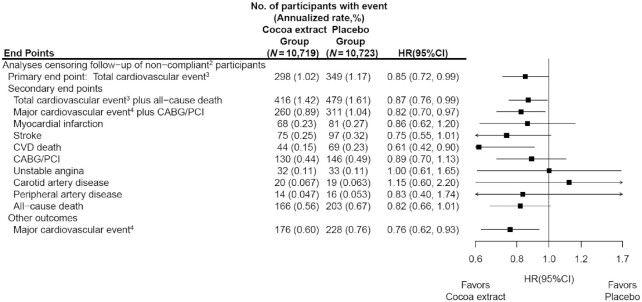
Results: During a median follow-up of 3.6 y, 410 participants taking cocoa extract and 456 taking placebo had confirmed total cardiovascular events (HR: 0.90; 95% CI: 0.78, 1.02; P = 0.11). For secondary endpoints, HRs were 0.73 (95% CI: 0.54, 0.98) for CVD death, 0.87 (95% CI: 0.66, 1.16) for MI, 0.91 (95% CI: 0.70, 1.17) for stroke, 0.95 (95% CI: 0.77, 1.17) for coronary revascularization, neutral for other individual cardiovascular endpoints, and 0.89 (95% CI: 0.77, 1.03) for all-cause mortality. Per-protocol analyses censoring follow-up at nonadherence supported a lower risk of total cardiovascular events (HR: 0.85; 95% CI: 0.72, 0.99). There were no safety concerns.
Conclusions: Cocoa extract supplementation did not significantly reduce total cardiovascular events among older adults but reduced CVD death by 27%. Potential reductions in total cardiovascular events were supported in per-protocol analyses. Additional research is warranted to clarify whether cocoa extract may reduce clinical cardiovascular events. This trial is registered at www.clinicaltrials.gov as NCT02422745.
Keywords: cancer; cardiovascular disease; cocoa extract; flavanols; multivitamin; randomized clinical trial.
© The Author(s) 2022. Published by Oxford University Press on behalf of the American Society for Nutrition.
Figures
Comment in
-
Bias attributable to the use of a composite outcome in evaluating a cocoa extract supplement.Am J Clin Nutr. 2022 Nov;116(5):1452. doi: 10.1093/ajcn/nqac185. Epub 2023 Feb 10. Am J Clin Nutr. 2022. PMID: 35776948 No abstract available.
References
-
- Dillinger TL, Barriga P, Escarcega S, Jimenez M, Salazar Lowe D, Grivetti LE. Food of the gods: cure for humanity? A cultural history of the medicinal and ritual use of chocolate. J Nutr. 2000;130(8):2057S–72S. - PubMed
-
- Aron PM, Kennedy JA. Flavan-3-ols: nature, occurrence and biological activity. Mol Nutr Food Res. 2008;52(1):79–104. - PubMed
-
- Onatibia-Astibia A, Franco R, Martinez-Pinilla E. Health benefits of methylxanthines in neurodegenerative diseases. Mol Nutr Food Res. 2017;61(6):2001600670–201600884.. doi:10.1002/mnfr.201600670. - PubMed
-
- Sansone R, Ottaviani JI, Rodriguez-Mateos A, Heinen Y, Noske D, Spencer JP, Crozier A, Merx MW, Kelm M, Schroeter Het al. Methylxanthines enhance the effects of cocoa flavanols on cardiovascular function: randomized, double-masked controlled studies. Am J Clin Nutr. 2017;105(2):352–60. - PubMed
-
- Buijsse B, Weikert C, Drogan D, Bergmann M, Boeing H. Chocolate consumption in relation to blood pressure and risk of cardiovascular disease in German adults. Eur Heart J. 2010;31(13):1616–23. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
