

Novel volumetric capnography indices measure ventilation inhomogeneity in cystic fibrosis
- PMID: 35295235
- PMCID: PMC8918935
- DOI: 10.1183/23120541.00440-2021
Novel volumetric capnography indices measure ventilation inhomogeneity in cystic fibrosis
Abstract
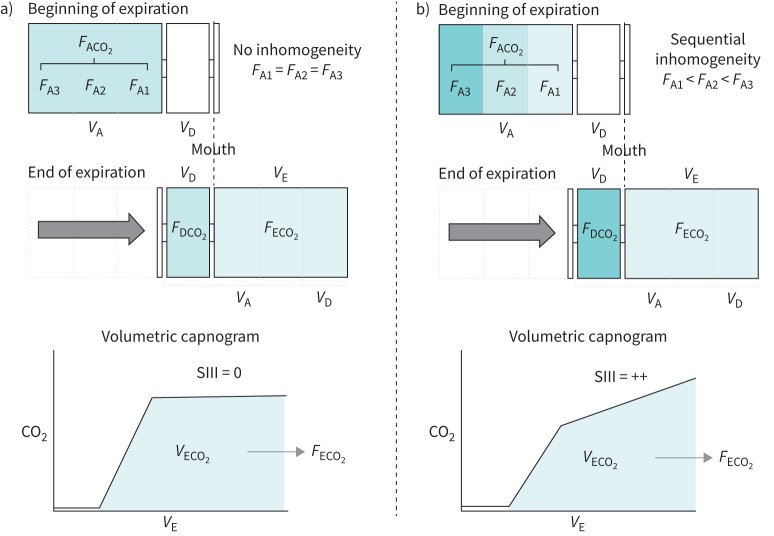
Background: Volumetric capnography (VCap) is a simpler alternative to multiple-breath washout (MBW) to detect ventilation inhomogeneity in patients with cystic fibrosis (CF). However, its diagnostic performance is influenced by breathing dynamics. We introduce two novel VCap indices, the capnographic inhomogeneity indices (CIIs), that may overcome this limitation and explore their diagnostic characteristics in a cohort of CF patients.
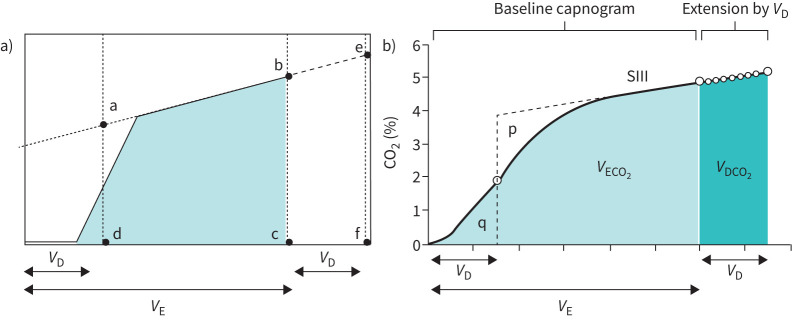
Methods: We analysed 320 N2-MBW trials from 50 CF patients and 65 controls (age 4-18 years) and calculated classical VCap indices, such as slope III (SIII) and the capnographic index (KPIv). We introduced novel CIIs based on a theoretical lung model and assessed their diagnostic performance compared to classical VCap indices and the lung clearance index (LCI).
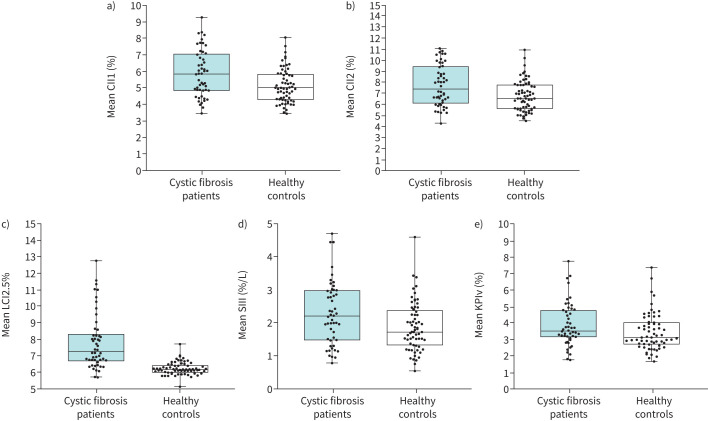
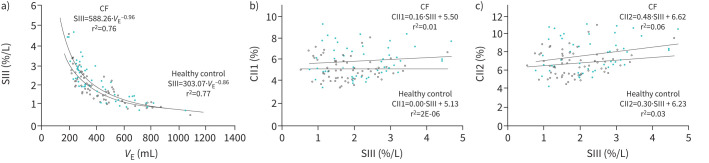
Results: Both CIIs were significantly higher in CF patients compared with controls (mean±sd CII1 5.9±1.4% versus 5.1±1.0%, p=0.002; CII2 7.7±1.8% versus 6.8±1.4%, p=0.002) and presented strong correlation with LCI (CII1 r2=0.47 and CII2 r2=0.44 in CF patients). Classical VCap indices showed inferior discriminative ability (SIII 2.3±1.0%/L versus 1.9±0.7%/L, p=0.013; KPIv 3.9±1.3% versus 3.5±1.2%, p=0.071), while the correlation with LCI was weak (SIII r2=0.03; KPIv r2=0.08 in CF patients). CIIs showed lower intra-subject inter-trial variability, calculated as coefficient of variation for three and relative difference for two trials, than classical VCap indices, but higher than LCI (CII1 11.1±8.2% and CII2 11.0±8.0% versus SIII 16.3±13.5%; KPIv 15.9±12.8%; LCI 5.9%±4.2%).
Conclusion: CIIs detect ventilation inhomogeneity better than classical VCap indices and correlate well with LCI. However, further studies on their diagnostic performance and clinical utility are required.
Copyright ©The authors 2022.
Conflict of interest statement
Conflicts of interest: S. Fouzas has nothing to disclose. Conflicts of interest: A-C. Kentgens repots no other conflicts of interest. Conflicts of interest: O. Lagiou has nothing to disclose. Conflicts of interest: B.S. Frauchiger has nothing to disclose. Conflicts of interest: F. Wyler has nothing to disclose. Conflicts of interest: I. Theodorakopoulos has nothing to disclose. Conflicts of interest: S. Yammine repots no other conflicts of interest. Conflicts of interest: P. Latzin reports grants from Vertex and Vifor paid to his institution, personal fees and honoraria paid to his institution from Vertex, Vifor and OM Pharma, fees for participation on a data safety monitoring or advisory board from Santhera (DMC), and personal fees paid to his institution from Polyphor, Vertex, OM pharma and Vifor, all outside the submitted work. Support statement: The work was supported by Swiss National Science Foundation Grants (Yammine 179905 and Latzin 182719). A-C. Kentgens is a recipient of the Swiss Government Excellence Scholarship from The Swiss Confederation. Funding information for this article has been deposited with the Crossref Funder Registry.
Figures
Similar articles
-
Calculation of the capnographic index based on expiratory molar mass-volume-curves--a suitable tool to screen for cystic fibrosis lung disease.J Cyst Fibros. 2013 May;12(3):277-83. doi: 10.1016/j.jcf.2012.08.011. Epub 2012 Sep 12. J Cyst Fibros. 2013. PMID: 22981527
-
Abnormal Lung Clearance Index in Cystic Fibrosis Children with Normal FEV1 and Single-Breath Nitrogen Washout Test.Lung. 2021 Feb;199(1):37-41. doi: 10.1007/s00408-020-00412-8. Epub 2021 Jan 3. Lung. 2021. PMID: 33389068
-
Limitations of regional ventilation inhomogeneity indices in children with cystic fibrosis.Pediatr Pulmonol. 2020 Sep;55(9):2315-2322. doi: 10.1002/ppul.24863. Epub 2020 Jun 1. Pediatr Pulmonol. 2020. PMID: 32441886
-
[Lung clearance index in cystic fibrosis].Rev Mal Respir. 2019 Mar;36(3):377-395. doi: 10.1016/j.rmr.2018.03.007. Epub 2019 Jan 25. Rev Mal Respir. 2019. PMID: 30686561 Review. French.
-
Applications of lung clearance index in monitoring children with cystic fibrosis.World J Clin Pediatr. 2019 Apr 9;8(2):15-22. doi: 10.5409/wjcp.v8.i2.15. eCollection 2019 Apr 9. World J Clin Pediatr. 2019. PMID: 31041164 Free PMC article. Review.
Cited by
-
ERS International Congress 2022: highlights from the Paediatrics Assembly.ERJ Open Res. 2023 May 22;9(3):00653-2022. doi: 10.1183/23120541.00653-2022. eCollection 2023 May. ERJ Open Res. 2023. PMID: 37228264 Free PMC article. Review.
-
Evaluation of the Double-Tracer Gas Single-Breath Washout Test in a Pediatric Field Study.Chest. 2024 Feb;165(2):396-404. doi: 10.1016/j.chest.2023.09.006. Epub 2023 Sep 15. Chest. 2024. PMID: 37716474 Free PMC article.
References
LinkOut - more resources
Full Text Sources