

Segmental Chiropractic Spinal Manipulation Does not Reduce Pain Amplification and the Associated Pain-Related Brain Activity in a Capsaicin-Heat Pain Model
- PMID: 35295444
- PMCID: PMC8915690
- DOI: 10.3389/fpain.2021.733727
Segmental Chiropractic Spinal Manipulation Does not Reduce Pain Amplification and the Associated Pain-Related Brain Activity in a Capsaicin-Heat Pain Model
Abstract
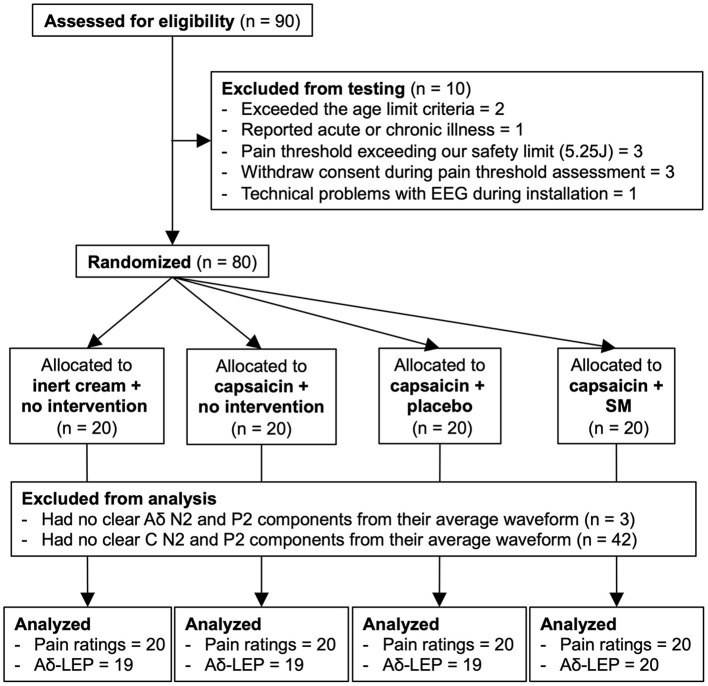
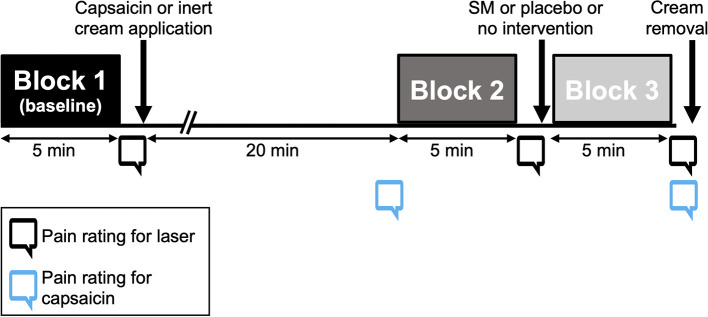
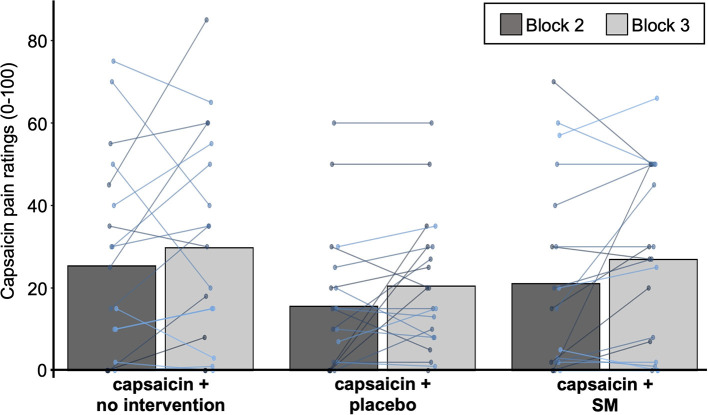
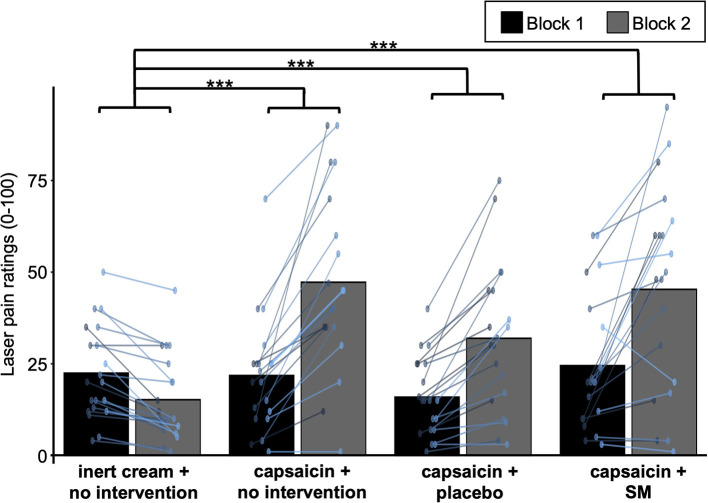
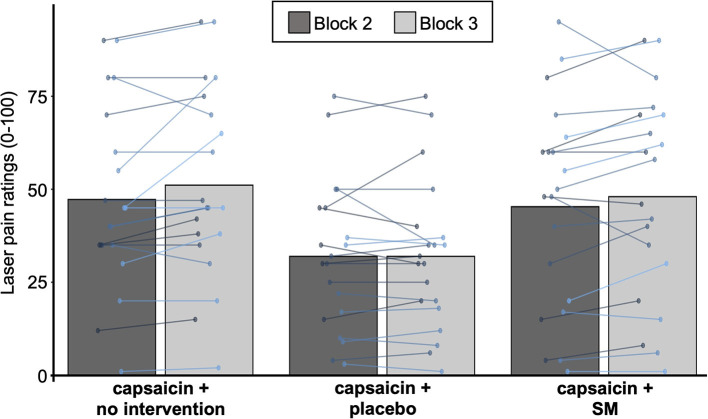
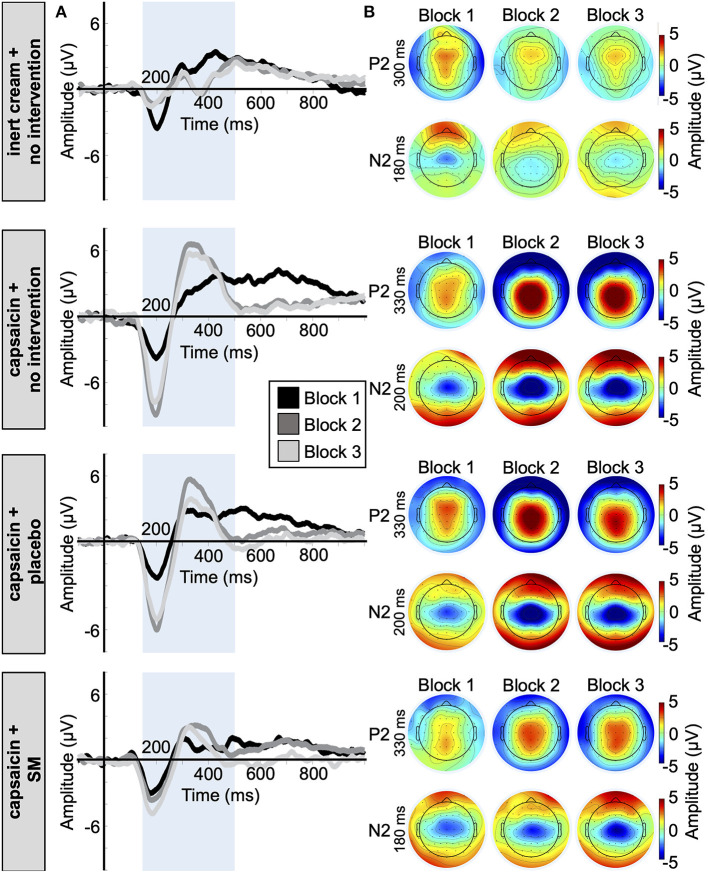
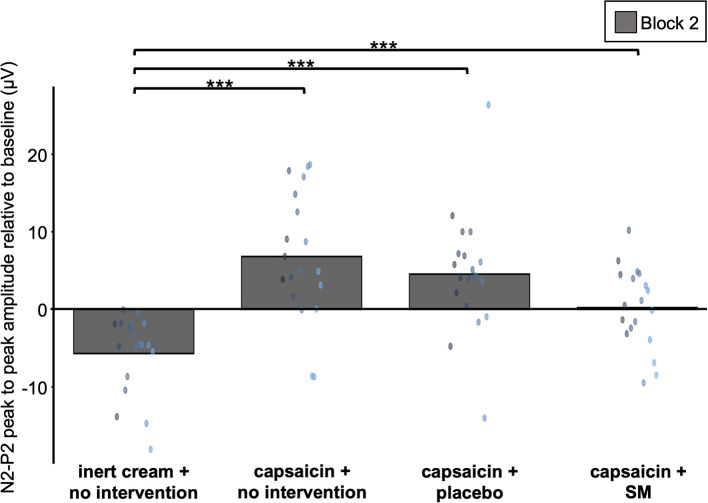
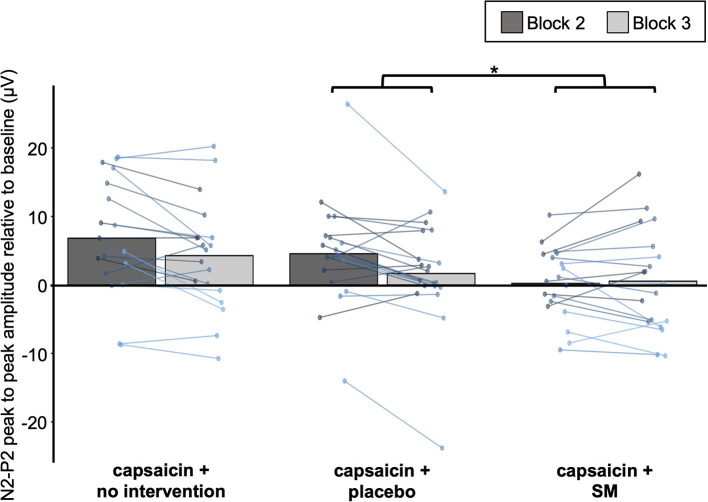
Musculoskeletal injuries lead to sensitization of nociceptors and primary hyperalgesia (hypersensitivity to painful stimuli). This occurs with back injuries, which are associated with acute pain and increased pain sensitivity at the site of injury. In some cases, back pain persists and leads to central sensitization and chronic pain. Thus, reducing primary hyperalgesia to prevent central sensitization may limit the transition from acute to chronic back pain. It has been shown that spinal manipulation (SM) reduces experimental and clinical pain, but the effect of SM on primary hyperalgesia and hypersensitivity to painful stimuli remains unclear. The goal of the present study was to investigate the effect of SM on pain hypersensitivity using a capsaicin-heat pain model. Laser stimulation was used to evoke heat pain and the associated brain activity, which were measured to assess their modulation by SM. Eighty healthy participants were recruited and randomly assigned to one of the four experimental groups: inert cream and no intervention; capsaicin cream and no intervention; capsaicin cream and SM at T7; capsaicin cream and placebo. Inert or capsaicin cream (1%) was applied to the T9 area. SM or placebo were performed 25 min after cream application. A series of laser stimuli were delivered on the area of cream application (1) before cream application, (2) after cream application but before SM or placebo, and (3) after SM or placebo. Capsaicin cream induced a significant increase in laser pain (p < 0.001) and laser-evoked potential amplitude (p < 0.001). However, SM did not decrease the amplification of laser pain or laser-evoked potentials by capsaicin. These results indicate that segmental SM does not reduce pain hypersensitivity and the associated pain-related brain activity in a capsaicin-heat pain model.
Keywords: SMT; manual therapy; pain; pain modulation; spine.
Copyright © 2021 Provencher, Northon and Piché.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Chiropractic Spinal Manipulation Prevents Secondary Hyperalgesia Induced by Topical Capsaicin in Healthy Individuals.Front Pain Res (Lausanne). 2021 Jul 20;2:702429. doi: 10.3389/fpain.2021.702429. eCollection 2021. Front Pain Res (Lausanne). 2021. PMID: 35295504 Free PMC article.
-
Effects of chiropractic spinal manipulation on laser-evoked pain and brain activity.J Physiol Sci. 2021 Jun 24;71(1):20. doi: 10.1186/s12576-021-00804-2. J Physiol Sci. 2021. PMID: 34167458 Free PMC article. Clinical Trial.
-
Pain, hyperalgesia and activity in nociceptive C units in humans after intradermal injection of capsaicin.J Physiol. 1992 Mar;448:749-64. doi: 10.1113/jphysiol.1992.sp019068. J Physiol. 1992. PMID: 1593488 Free PMC article.
-
Peripheral and central mechanisms of cutaneous hyperalgesia.Prog Neurobiol. 1992;38(4):397-421. doi: 10.1016/0301-0082(92)90027-c. Prog Neurobiol. 1992. PMID: 1574584 Review.
-
Neurophysiological mechanisms of chiropractic spinal manipulation for spine pain.Eur J Pain. 2021 Aug;25(7):1429-1448. doi: 10.1002/ejp.1773. Epub 2021 Apr 15. Eur J Pain. 2021. PMID: 33786932 Review.
Cited by
-
Incidence and predictors of residual back pain after percutaneous vertebral augmentation in osteoporotic vertebral compression fracture: a systematic review and meta analysis.Osteoporos Int. 2025 Jul 23. doi: 10.1007/s00198-025-07609-8. Online ahead of print. Osteoporos Int. 2025. PMID: 40699245 Review.
-
A modern way to teach and practice manual therapy.Chiropr Man Therap. 2024 May 21;32(1):17. doi: 10.1186/s12998-024-00537-0. Chiropr Man Therap. 2024. PMID: 38773515 Free PMC article. Review.
-
C-fiber-related brain responses evoked by laser heat pulses applied to the back.J Physiol Sci. 2025 Jul;75(2):100018. doi: 10.1016/j.jphyss.2025.100018. Epub 2025 Mar 24. J Physiol Sci. 2025. PMID: 40158365 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Medical