

Sensitivity and Specificity of MRI in Diagnosing Concomitant Meniscal Injuries With Pediatric and Adolescent Acute ACL Tears
- PMID: 35295551
- PMCID: PMC8918745
- DOI: 10.1177/23259671221079338
Sensitivity and Specificity of MRI in Diagnosing Concomitant Meniscal Injuries With Pediatric and Adolescent Acute ACL Tears
Abstract
Background: Preoperative diagnosis of concomitant meniscal tears in pediatric and adolescent patients with acute anterior cruciate ligament (ACL) deficiency is challenging.
Purpose: To investigate the diagnostic performance of magnetic resonance imaging (MRI) in detecting meniscal injuries for pediatric and adolescent patients with acute ACL tears.
Study design: Cohort study (diagnosis); Level of evidence, 2.
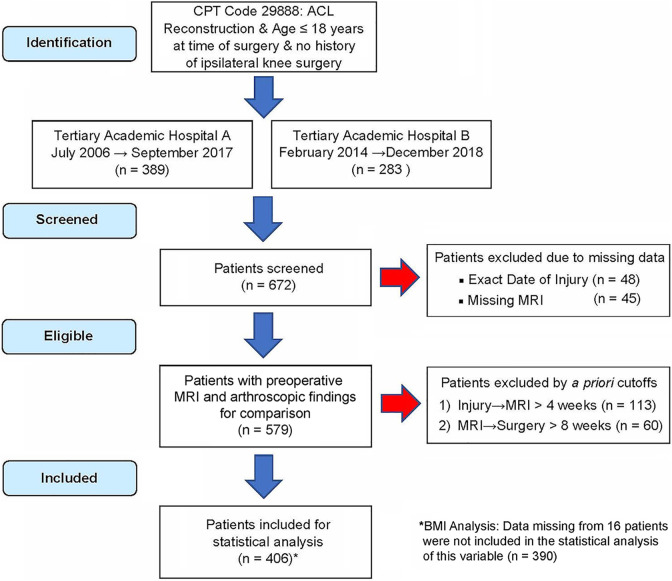
Methods: The authors retrospectively identified patients aged ≤18 years who underwent acute ACL reconstruction between 2006 and 2018 at 2 tertiary academic hospitals. The primary outcomes were arthroscopically confirmed medial, lateral, or any (defined as medial and/or lateral) meniscal tears. To control for chronically deficient knees, patients must have received their MRI study within 4 weeks of injury and must have undergone surgery no more than 8 weeks after their MRI study. Preoperative MRI reports were compared with the gold standard of arthroscopically confirmed tears to calculate sensitivity, specificity, positive predictive value, and negative predictive value. In a secondary analysis, patients were stratified by age into 2 groups (≤13 or ≥14 years), body mass index-for-age data from the Centers for Disease Control were used to classify patients as obese or nonobese, and differences between sensitivity and specificity proportions were analyzed using chi-square test for homogeneity.
Results: Overall, 406 patients with a mean age of 15.4 years (range, 10-18 years) were identified. The sensitivity, specificity, positive predictive value, and negative predictive value were as follows: for lateral meniscal (LM) tears, 51.0%, 86.5%, 78.3%, and 65.0%; for medial meniscal tears, 83.2%, 80.6%, 62.3%, and 92.5%; and for any meniscal tear, 75.0%, 72.1%, 81.5%, and 63.8%, respectively. In the stratified analysis, MRI was less specific for the following diagnoses: any meniscal tear in patients aged ≤13 years (P = .048) and LM tears in obese patients (P = .020).
Conclusion: The diagnostic ability of MRI to predict meniscal injuries present at acute ACL reconstruction was moderate. Performance was poorest at the lateral meniscus, where MRI failed to detect 97 tears that were found arthroscopically. Specificity was significantly lower in younger patients for any meniscal tear and in obese patients for LM tears.
Keywords: MRI; adolescent; meniscus; pediatric; sensitivity; specificity.
© The Author(s) 2022.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: P.D.F. has received hospitality payments from Medical Device Business Services. A.G. has received education payments from Arthrex. M.S. has received consulting fees and royalties from OrthoPediatrics and hospitality payments from Stryker. R.J.M. has received education payments from Arthrex, consulting fees from Medical Device Business Services and OrthoPediatrics, speaking fees from Philips Electronic North America, and hospitality payments from Globus Medical and Medical Device Business Services. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
Confirming the Presence of Unrecognized Meniscal Injuries on Magnetic Resonance Imaging in Pediatric and Adolescent Patients With Anterior Cruciate Ligament Tears.J Pediatr Orthop. 2019 Oct;39(9):e661-e667. doi: 10.1097/BPO.0000000000001331. J Pediatr Orthop. 2019. PMID: 30628976
-
Efficacy of magnetic resonance imaging evaluation for meniscal tear in acute anterior cruciate ligament injuries.Arthroscopy. 2014 Apr;30(4):475-82. doi: 10.1016/j.arthro.2013.12.016. Arthroscopy. 2014. PMID: 24680307
-
Effect of Increased Time to Surgery on the Ability of MRI to Rule Out Medial Meniscal Tears in Young Athletes With ACL Injury.Orthop J Sports Med. 2023 Jan 27;11(1):23259671221141664. doi: 10.1177/23259671221141664. eCollection 2023 Jan. Orthop J Sports Med. 2023. PMID: 36743735 Free PMC article.
-
Associated injuries in pediatric and adolescent anterior cruciate ligament tears: does a delay in treatment increase the risk of meniscal tear?Arthroscopy. 2002 Nov-Dec;18(9):955-9. doi: 10.1053/jars.2002.36114. Arthroscopy. 2002. PMID: 12426537 Review.
-
Early Operative Versus Delayed Operative Versus Nonoperative Treatment of Pediatric and Adolescent Anterior Cruciate Ligament Injuries: A Systematic Review and Meta-analysis.Am J Sports Med. 2021 Dec;49(14):4008-4017. doi: 10.1177/0363546521990817. Epub 2021 Mar 15. Am J Sports Med. 2021. PMID: 33720764
Cited by
-
Magnetic Resonance Imaging Is an Effective First-Line Noninvasive Tool for Meniscal Tear Detection: A Retrospective Comparative Analysis With Knee Arthroscopy.Arthrosc Sports Med Rehabil. 2024 Dec 12;7(2):101065. doi: 10.1016/j.asmr.2024.101065. eCollection 2025 Apr. Arthrosc Sports Med Rehabil. 2024. PMID: 40297094 Free PMC article.
-
High Detection Rate of Posterolateral Tibial Plateau Fractures and Poor Functional Outcomes in Type IIIB Impaction Fractures After Anterior Cruciate Ligament Rupture and Reconstruction.Orthop Surg. 2025 Apr;17(4):1086-1094. doi: 10.1111/os.14358. Epub 2025 Jan 18. Orthop Surg. 2025. PMID: 39825704 Free PMC article.
-
Arthroscopy-validated diagnostic performance of sub-5-min deep learning super-resolution 3T knee MRI in children and adolescents.Skeletal Radiol. 2025 Jun 10. doi: 10.1007/s00256-025-04969-4. Online ahead of print. Skeletal Radiol. 2025. PMID: 40493057
-
The Role of Crutches and Bracing in Preventing Secondary Meniscal Tears After Anterior Cruciate Ligament Injury in Pediatric Patients.Orthop J Sports Med. 2025 Feb 6;13(2):23259671241309862. doi: 10.1177/23259671241309862. eCollection 2025 Feb. Orthop J Sports Med. 2025. PMID: 39944767 Free PMC article.
-
Analysis of Discordant Findings between 3T Magnetic Resonance Imaging and Arthroscopic Evaluation of the Knee Meniscus.J Clin Med. 2023 Aug 31;12(17):5667. doi: 10.3390/jcm12175667. J Clin Med. 2023. PMID: 37685734 Free PMC article.
References
-
- Anderson AF, Anderson CN. Correlation of meniscal and articular cartilage injuries in children and adolescents with timing of anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43(2):275–281. doi:10.1177/0363546514559912 - PubMed
-
- Bouju Y, Carpentier E, Bergerault F, de Courtivron B, Bonnard C, Garaud P. The concordance of MRI and arthroscopy in traumatic meniscal lesions in children. Orthop Traumatol Surg Res. 2011;97(7):712–718. doi:10.1016/j.otsr.2011.07.010 - PubMed
-
- Centers for Disease Control and Prevention. Clinical Growth Charts. https://www.cdc.gov/growthcharts/clinical_charts.htm
-
- Church S, Keating JF. Reconstruction of the anterior cruciate ligament: timing of surgery and the incidence of meniscal tears and degenerative change. J Bone Joint Surg Br. 2005;87(12):1639–1642. doi:10.1302/0301-620X.87B12.16916 - PubMed
-
- Clark CR, Ogden JA. Development of the menisci of the human knee joint. J Bone Joint Surg Am. 1983;65(4):538–547. - PubMed
LinkOut - more resources
Full Text Sources
