

Efficacy and Safety of Radiofrequency Ablation vs. Endoscopic Surveillance for Barrett's Esophagus With Low-Grade Dysplasia: Meta-Analysis of Randomized Controlled Trials
- PMID: 35296005
- PMCID: PMC8920305
- DOI: 10.3389/fonc.2022.801940
Efficacy and Safety of Radiofrequency Ablation vs. Endoscopic Surveillance for Barrett's Esophagus With Low-Grade Dysplasia: Meta-Analysis of Randomized Controlled Trials
Abstract
Background and aims: Barrett's esophagus with low-grade dysplasia (BE-LGD) carries a risk of progression to Barrett's esophagus with high-grade dysplasia (BE-HGD) and esophageal adenocarcinoma (EAC). Radiofrequency ablation (RFA) appears to be a safe and efficacious method to eradicate Barrett's esophagus. However, a confirmed consensus regarding treatment of BE-LGD with RFA vs. endoscopic surveillance is lacking. Therefore, this study aimed to elucidate the efficacy and safety for RFA vs. endoscopic surveillance in decreasing the risk of BE-LGD progression to BE-HGD or EAC.
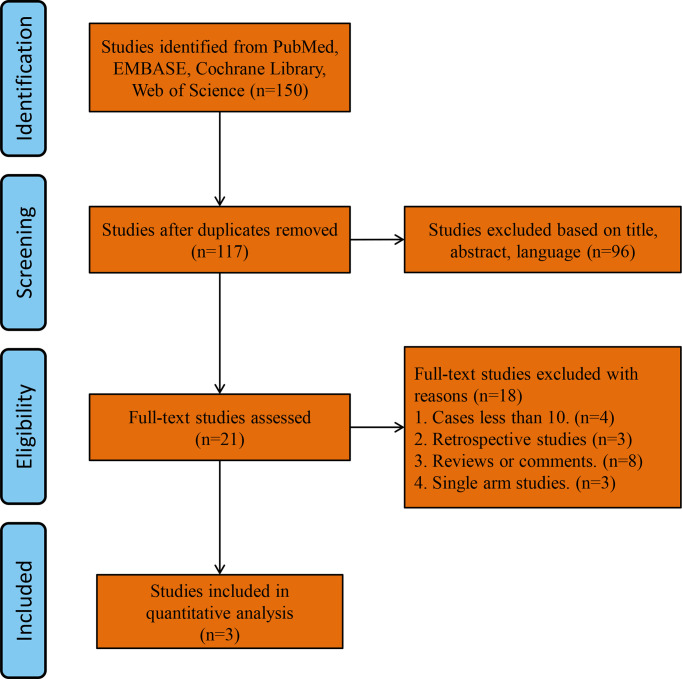
Methods: Relevant studies published before May 1, 2021 were identified by searching relevant medical databases. The primary outcome was the rate of progression BE-LGD to HGD and/or EAC after treatment with RFA and endoscopic surveillance. The secondary outcome was the rate of complete eradication of dysplasia (CE-D) and complete eradication of intestinal metaplasia (CE-IM) after treatment with RFA and endoscopic surveillance. Adverse events were also extracted and evaluated.
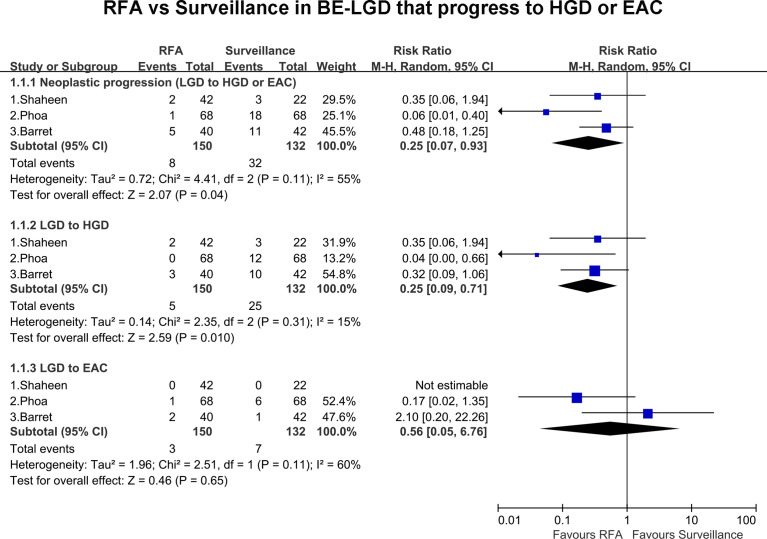
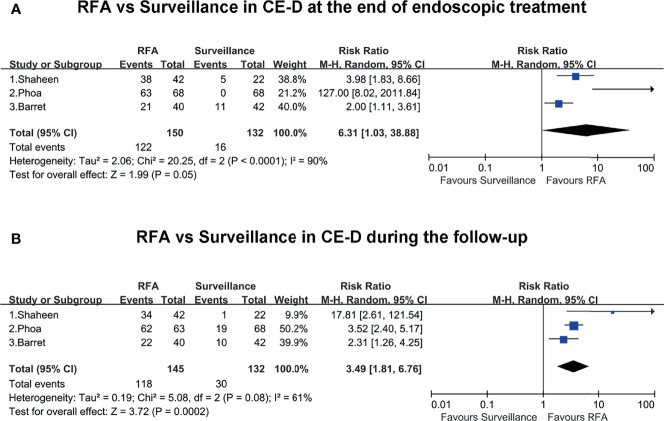
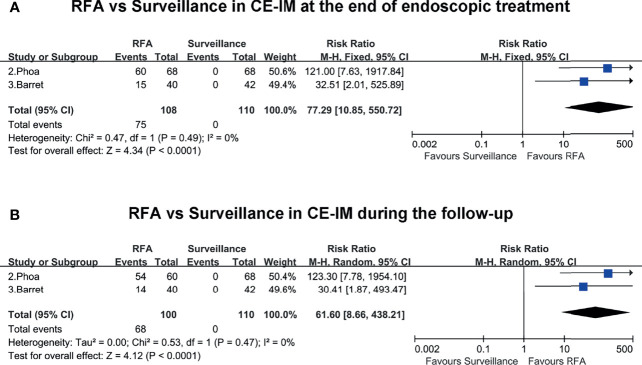
Results: Three randomized controlled trials were eligible for analysis. The pooled estimate of rate of neoplastic progression of BE-LGD to HGD or EAC was much lower in the RFA group than the endoscopic surveillance group (RR, 0.25; 95% CI, 0.07-0.93; P = 0.04), with moderate heterogeneity (I2 = 55%). Subgroup analysis based on progression grade was performed. The pooled rate of progression of BE-LGD to HGD was much lower in the RFA group than the endoscopic surveillance group (RR, 0.25; 95% CI, 0.07-0.71; P = 0.01), with low heterogeneity (I2 = 15%). Although the pooled risk of progression of BE-LGD to EAC was slightly lower in the RFA group than the endoscopic surveillance group (RR, 0.56; 95% CI, 0.05-6.76), the result was not statistically significant (P = 0.65). RFA also was associated a higher rate of CE-D and CE-IM both at the end of endoscopic treatment and during follow-up. However, the rate of adverse events was slightly higher after RFA treatment.
Conclusion: RFA decreases the risk of BE-LGD progression to BE-HGD. However, given the uncertain course of LGD and the potential for esophageal stricture after RFA, treatment options should be fully considered and weighed.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021266128, identifier PROSPERO (CRD42021266128).
Keywords: Barrett’s esophagus; endoscopic surveillance; esophageal adenocarcinoma (EAC); high-grade dysplasia (HGD); low-grade dysplasia (LGD); radiofrequency ablation.
Copyright © 2022 Wang, Ma, Yang, Li and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Outcomes of Radiofrequency Ablation versus Endoscopic Surveillance for Barrett's Esophagus with Low-Grade Dysplasia: A Systematic Review and Meta-Analysis.Dig Dis. 2021;39(6):561-568. doi: 10.1159/000514786. Epub 2021 Jan 27. Dig Dis. 2021. PMID: 33503615
-
Efficacy and durability of radiofrequency ablation for Barrett's Esophagus: systematic review and meta-analysis.Clin Gastroenterol Hepatol. 2013 Oct;11(10):1245-55. doi: 10.1016/j.cgh.2013.03.039. Epub 2013 May 2. Clin Gastroenterol Hepatol. 2013. PMID: 23644385 Free PMC article.
-
Radiofrequency Ablation Is Associated With Decreased Neoplastic Progression in Patients With Barrett's Esophagus and Confirmed Low-Grade Dysplasia.Gastroenterology. 2015 Sep;149(3):567-76.e3; quiz e13-4. doi: 10.1053/j.gastro.2015.04.013. Epub 2015 Apr 24. Gastroenterology. 2015. PMID: 25917785 Free PMC article.
-
The cost effectiveness of radiofrequency ablation for Barrett's esophagus.Gastroenterology. 2012 Sep;143(3):567-575. doi: 10.1053/j.gastro.2012.05.010. Epub 2012 May 21. Gastroenterology. 2012. PMID: 22626608 Free PMC article.
-
Radio frequency ablation of dysplastic Barrett's esophagus: Outcomes of a single-center registry.Scand J Surg. 2023 Jun;112(2):86-90. doi: 10.1177/14574969231151378. Epub 2023 Feb 8. Scand J Surg. 2023. PMID: 36756673
Cited by
-
Endoscopic Management of Dysplastic Barrett's Oesophagus and Early Oesophageal Adenocarcinoma.Cancers (Basel). 2023 Sep 28;15(19):4776. doi: 10.3390/cancers15194776. Cancers (Basel). 2023. PMID: 37835470 Free PMC article. Review.
-
What Is "Cold" and What Is "Hot" in Mucosal Ablation for Barrett's Oesophagus-Related Dysplasia: A Practical Guide.Life (Basel). 2023 Apr 15;13(4):1023. doi: 10.3390/life13041023. Life (Basel). 2023. PMID: 37109552 Free PMC article. Review.
-
Factors influencing the cost-effectiveness of radiofrequency ablation for Barrett's esophagus with low-grade dysplasia in Australia.Dis Esophagus. 2025 Jan 7;38(1):doae095. doi: 10.1093/dote/doae095. Dis Esophagus. 2025. PMID: 39498762 Free PMC article.
-
Comparison of interventions for Barrett's esophagus: A network meta-analysis.PLoS One. 2024 May 6;19(5):e0302204. doi: 10.1371/journal.pone.0302204. eCollection 2024. PLoS One. 2024. PMID: 38709808 Free PMC article.
References
-
- van Vilsteren FG, Pouw RE, Seewald S, Alvarez Herrero L, Sondermeijer CM, Visser M, et al. . Stepwise Radical Endoscopic Resection Versus Radiofrequency Ablation for Barrett’s Oesophagus With High-Grade Dysplasia or Early Cancer: A Multicentre Randomised Trial. Gut (2011) 60:765–73. doi: 10.1136/gut.2010.229310 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources