

Use of nephrotoxic medications in adults with chronic kidney disease in Swedish and US routine care
- PMID: 35296039
- PMCID: PMC8922703
- DOI: 10.1093/ckj/sfab210
Use of nephrotoxic medications in adults with chronic kidney disease in Swedish and US routine care
Abstract
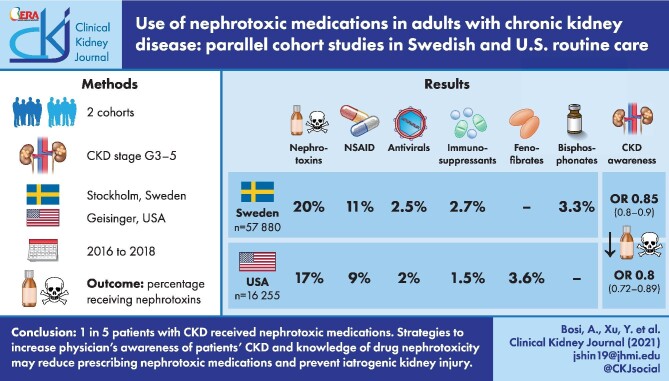
Background: To characterize the use of nephrotoxic medications in patients with chronic kidney disease (CKD) Stages G3-5 in routine care.
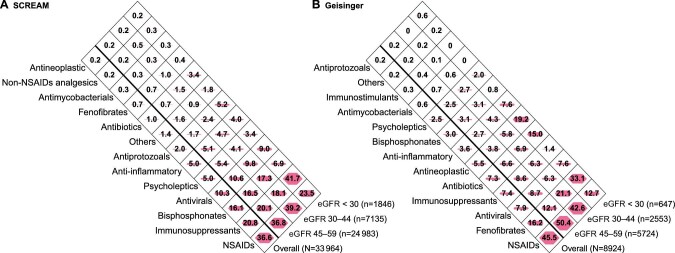
Methods: We studied cohorts of adults with confirmed CKD G3-5 undergoing routine care from 1 January 2016 through 31 December 2018 in two health systems [Stockholm CREAtinine Measurements (SCREAM), Stockholm, Sweden (N = 57 880) and Geisinger, PA, USA (N = 16 255)]. We evaluated the proportion of patients receiving nephrotoxic medications within 1 year overall and by baseline kidney function, ranked main contributors and examined the association between receipt of nephrotoxic medication and age, sex, CKD G-stages comorbidities and provider awareness of the patient's CKD using multivariable logistic regression.
Results: During a 1-year period, 20% (SCREAM) and 17% (Geisinger) of patients with CKD received at least one nephrotoxic medication. Among the top nephrotoxic medications identified in both cohorts were non-steroidal anti-inflammatory drugs (given to 11% and 9% of patients in SCREAM and Geisinger, respectively), antivirals (2.5% and 2.0%) and immunosuppressants (2.7% and 1.5%). Bisphosphonate use was common in SCREAM (3.3%) and fenofibrates in Geisinger (3.6%). Patients <65 years of age, women and those with CKD G3 were at higher risk of receiving nephrotoxic medications in both cohorts. Notably, provider awareness of a patient's CKD was associated with lower odds of nephrotoxic medication use {odds ratios [OR] 0.85[95% confidence interval (CI) 0.80-0.90] in SCREAM and OR 0.80 [95% CI 0.72-0.89] in Geisinger}.
Conclusions: One in five patients with CKD received nephrotoxic medications in two distinct health systems. Strategies to increase physician's awareness of patients' CKD and knowledge of drug nephrotoxicity may reduce prescribing nephrotoxic medications and prevent iatrogenic kidney injury.
Keywords: chronic kidney disease; estimated glomerular filtration rate; nephrotoxicity.
© The Author(s) 2021. Published by Oxford University Press on behalf of the ERA.
Figures

Comment on
-
More on the invisibility of chronic kidney disease… and counting.Clin Kidney J. 2021 Nov 27;15(3):388-392. doi: 10.1093/ckj/sfab240. eCollection 2022 Mar. Clin Kidney J. 2021. PMID: 35198154 Free PMC article.
-
RICORS2040: the need for collaborative research in chronic kidney disease.Clin Kidney J. 2021 Sep 23;15(3):372-387. doi: 10.1093/ckj/sfab170. eCollection 2022 Mar. Clin Kidney J. 2021. PMID: 35211298 Free PMC article.
References
-
- Classen DC, Pestotnik SL, Evans RSet al. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA 1997; 277: 301–306 - PubMed
-
- Budnitz DS, Pollock DA, Weidenbach KNet al. National surveillance of emergency department visits for outpatient adverse drug events. JAMA 2006; 296: 1858–1866 - PubMed
-
- Institute of Medicine . Preventing Medication Errors. Washington, DC: National Academies Press, 2007
-
- Office of Disease Prevention and Health Promotion . National Action Plan for Adverse Drug Event Prevention. Washington, DC: US Department of Health and Human Services, 2014
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
