

Effects of dynamic individualized PEEP guided by driving pressure in laparoscopic surgery on postoperative atelectasis in elderly patients: a prospective randomized controlled trial
- PMID: 35296253
- PMCID: PMC8925066
- DOI: 10.1186/s12871-022-01613-9
Effects of dynamic individualized PEEP guided by driving pressure in laparoscopic surgery on postoperative atelectasis in elderly patients: a prospective randomized controlled trial
Abstract
Background: Driving pressure (ΔP = Plateau pressure-PEEP) is highly correlated with postoperative pulmonary complications (PPCs) and appears to be a promising indicator for optimizing ventilator settings. We hypothesized that dynamic, individualized positive end-expiratory pressure (PEEP) guided by ΔP could reduce postoperative atelectasis and improve intraoperative oxygenation, respiratory mechanics, and reduce the incidence of PPCs on elderly patients undergoing laparoscopic surgery.
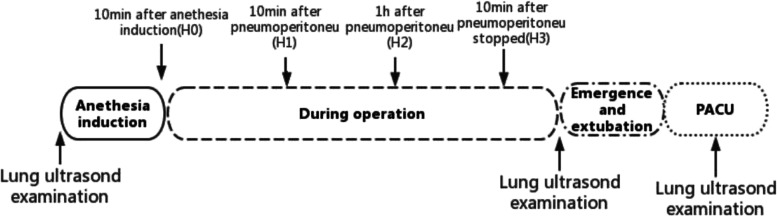
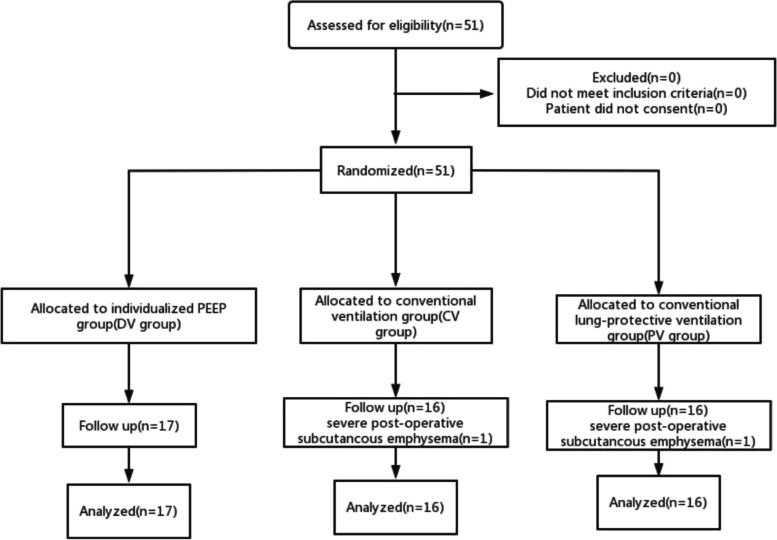
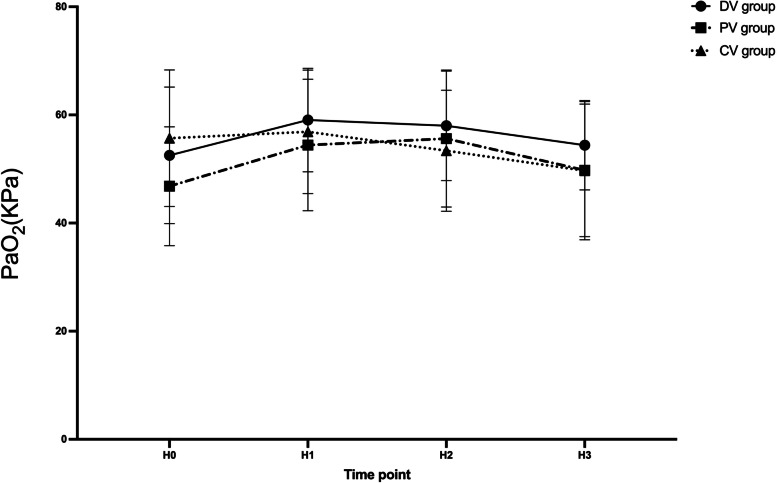
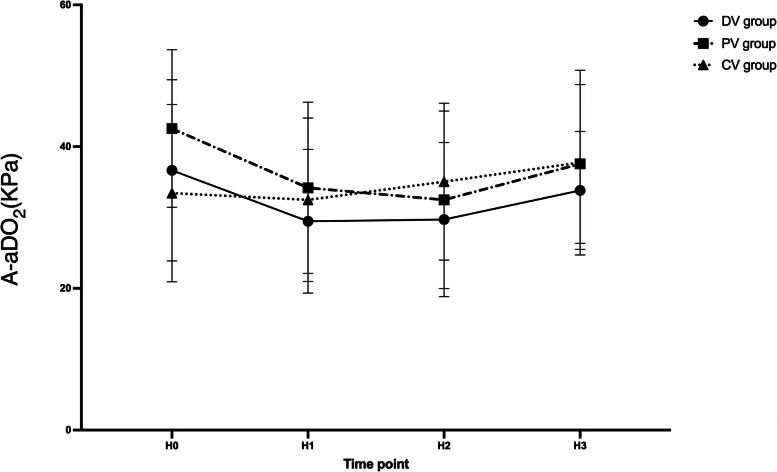
Methods: Fifty-one elderly patients who were subject to laparoscopic surgery participated in this randomized trial. In the PEEP titration group (DV group), the PEEP titration was decremented to the lowest ΔP and repeated every 1 h. Additional procedures were also performed when performing predefined events that may be associated with lung collapse. In the constant PEEP group (PV group), a PEEP of 6 cmH2O was used throughout the surgery. Moreover, zero PEEP was applied during the entire procedure in the conventional ventilation group (CV group). The primary objective of this study was lung ultrasound score noted at the end of surgery and 15 min after admission to the post-anesthesia care unit (PACU) at 12 lung areas bilaterally. The secondary endpoints were perioperative oxygenation function, expiratory mechanics, and the incidence of the PPCs.
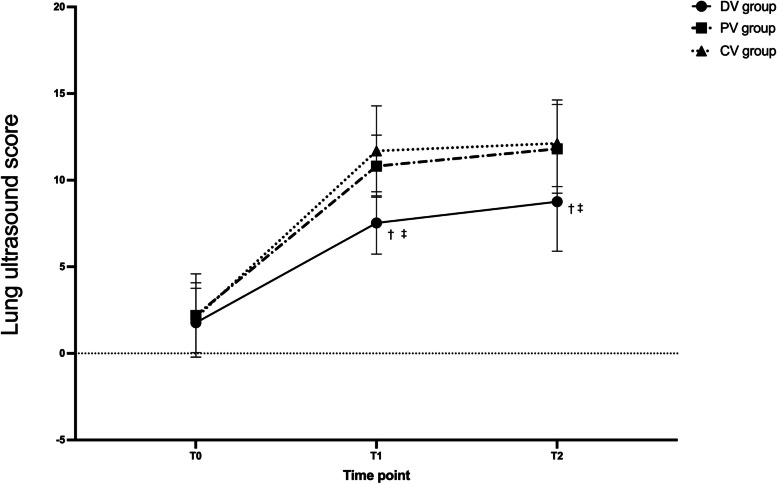
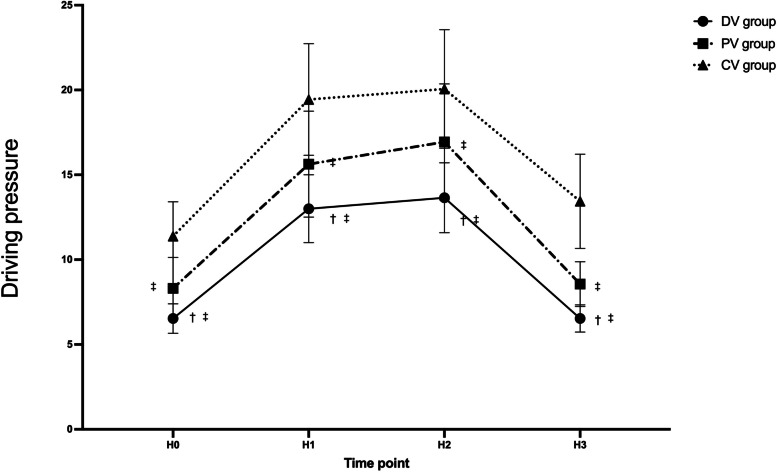
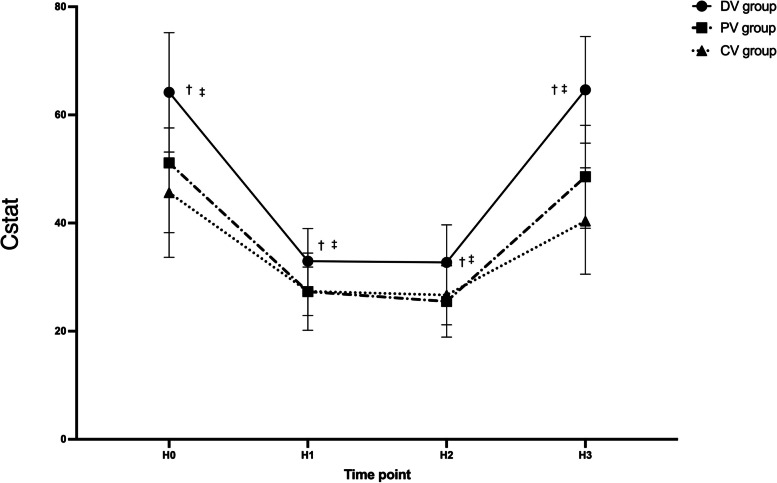
Results: The lung ultrasound scores of the DV group were significantly lower than those in the PV group and CV group (P < 0.05), whereas there was no significant difference between the PV group and CV group (P > 0.05). The lung static compliance (Cstat) and ΔP at all the intraoperative time points in the DV group were significantly better compared to the PV group and the CV group (p < 0.05).
Conclusions: Intraoperative titrated PEEP reduced postoperative lung atelectasis and improved respiratory mechanics in elderly patients undergoing laparoscopic surgery. Meanwhile, standard PEEP strategy is not superior to conventional ventilation in reducing postoperative pulmonary atelectasis in laparoscopic surgery.
Keywords: Atelectasis; Driving pressure; Laparoscopic surgery; Lung ultrasound; Positive end-expiratory pressure.
© 2022. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests.
Figures
Similar articles
-
Effect of driving pressure-guided individualized positive end-expiratory pressure (PEEP) ventilation strategy on postoperative atelectasis in patients undergoing laparoscopic surgery as assessed by ultrasonography: study protocol for a prospective randomized controlled trial.Trials. 2025 Mar 26;26(1):106. doi: 10.1186/s13063-025-08819-5. Trials. 2025. PMID: 40140868 Free PMC article.
-
Effects of intraoperative individualized PEEP on postoperative atelectasis in obese patients: study protocol for a prospective randomized controlled trial.Trials. 2020 Jul 6;21(1):618. doi: 10.1186/s13063-020-04565-y. Trials. 2020. PMID: 32631414 Free PMC article.
-
Effect of ultrasound-guided individualized positive end-expiratory pressure on the severity of postoperative atelectasis in elderly patients: a randomized controlled study.Sci Rep. 2024 Nov 15;14(1):28128. doi: 10.1038/s41598-024-79105-8. Sci Rep. 2024. PMID: 39548165 Free PMC article. Clinical Trial.
-
Individualized positive end-expiratory pressure guided by respiratory mechanics during anesthesia for the prevention of postoperative pulmonary complications: a systematic review and meta-analysis.J Clin Monit Comput. 2023 Apr;37(2):365-377. doi: 10.1007/s10877-022-00960-9. Epub 2023 Jan 6. J Clin Monit Comput. 2023. PMID: 36607532
-
Positive end-expiratory pressure and postoperative pulmonary complications in laparoscopic bariatric surgery: systematic review and meta-analysis.BMC Anesthesiol. 2024 Aug 9;24(1):282. doi: 10.1186/s12871-024-02658-8. BMC Anesthesiol. 2024. PMID: 39123102 Free PMC article.
Cited by
-
Laryngeal mask airway proseal versus laryngeal mask airway protector for laparoscopic surgery: A randomized comparative study.J Anaesthesiol Clin Pharmacol. 2025 Jul-Sep;41(3):532-537. doi: 10.4103/joacp.joacp_430_24. Epub 2025 Mar 22. J Anaesthesiol Clin Pharmacol. 2025. PMID: 40635823 Free PMC article.
-
Driving pressure-guided ventilation improves homogeneity in lung gas distribution for gynecological laparoscopy: a randomized controlled trial.Sci Rep. 2022 Dec 15;12(1):21687. doi: 10.1038/s41598-022-26144-8. Sci Rep. 2022. PMID: 36522433 Free PMC article. Clinical Trial.
-
Effect of driving pressure on early postoperative lung gas distribution in supratentorial craniotomy: a randomized controlled trial.BMC Anesthesiol. 2023 May 22;23(1):176. doi: 10.1186/s12871-023-02144-7. BMC Anesthesiol. 2023. PMID: 37217882 Free PMC article. Clinical Trial.
-
Driving pressure-guided dynamic PEEP titration reduces atelectasis and improves oxygenation in pediatric laparoscopy: a randomized trial on personalized ventilation strategies.BMC Anesthesiol. 2025 Aug 20;25(1):412. doi: 10.1186/s12871-025-03274-w. BMC Anesthesiol. 2025. PMID: 40835897 Free PMC article.
-
Driving pressure: A useful tool for reducing postoperative pulmonary complications.World J Crit Care Med. 2024 Sep 9;13(3):96214. doi: 10.5492/wjccm.v13.i3.96214. eCollection 2024 Sep 9. World J Crit Care Med. 2024. PMID: 39253315 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
