

Comorbidities in unclassifiable interstitial lung disease
- PMID: 35296320
- PMCID: PMC8925215
- DOI: 10.1186/s12931-022-01981-3
Comorbidities in unclassifiable interstitial lung disease
Abstract
Background: Comorbidities are common in interstitial lung diseases (ILD) and have an important association with survival, but the frequency and prognostic impact of comorbidities in unclassifiable interstitial lung disease (uILD) remains elusive. We aimed to describe the prevalence of comorbidities and assess the impact on survival in patients with uILD. Furthermore, we aimed to identify and characterize potential phenotypes based on clusters of comorbidities and examine their association with disease progression and survival.
Methods: Incident patients diagnosed with uILD were identified at two ILD referral centers in Denmark and Germany from 2003 to 2018. The diagnosis uILD was based on multidisciplinary team meetings. Clinical characteristics and comorbidities were extracted from ILD registries and patient case files. Survival analyses were performed using Cox regression analyses, disease progression was analyzed by linear mixed effects models, and clusters of comorbidities were analyzed using self-organizing maps.
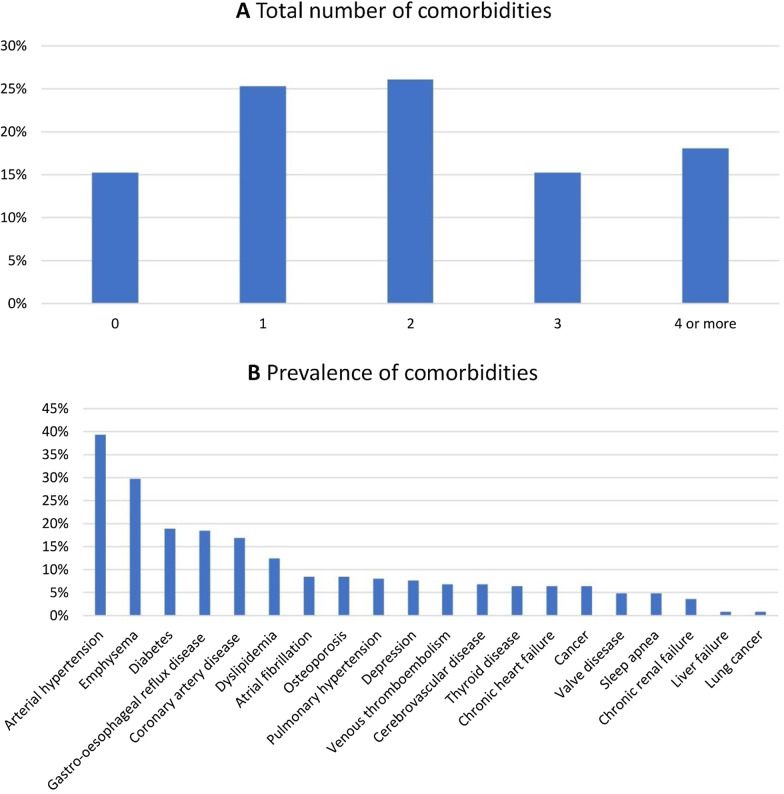
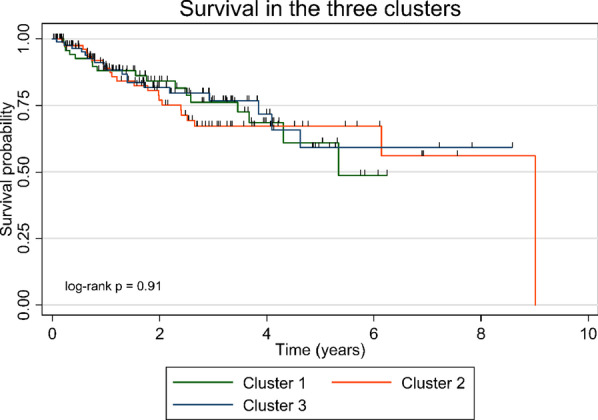
Results: A total of 249 patients with uILD were identified. The cohort was dominated by males (60%), former (49%) or current (15%) smokers, median age was 70 years, mean FVC was 75.9% predicted, and mean DLCO was 49.9% predicted. One-year survival was 89% and three-year survival was 73%. Eighty-five percent of the patients had ≥ 1 comorbidities, 33% had ≥ 3 comorbidities and 9% had ≥ 5 comorbidities. The only comorbidity associated with excess mortality was dyslipidemia. No association between survival and number of comorbidities or the Charlson comorbidity index was observed. Three clusters with different comorbidities profiles and clinical characteristics were identified. A significant annual decline in FVC and DLCO % predicted was observed in cluster 1 and 2, but not in cluster 3. No difference in mortality was observed between the clusters.
Conclusions: The comorbidity burden in uILD is lower than reported in other types of ILD and the impact of comorbidities on mortality needs further clarification. Three clusters with distinct comorbidity profiles were identified and could represent specific phenotypes. No difference in mortality was observed between clusters, but slower disease progression was observed in cluster 3. Better understanding of disease behavior and mortality will require further studies of subgroups of uILD with longer observation time.
Keywords: Cluster analyses; Comorbidities; Disease course; Mortality; Unclassifiable interstitial lung disease.
© 2022. The Author(s).
Conflict of interest statement
TSP reports personal fees from Galapagos, and grants and personal fees from Boehringer Ingelheim outside the submitted work; SKW reports grants from Roche during the conduct of the study, and personal fees from Roche and Bohringer Ingelheim outside the submitted work; EB reports grants from Roche during the conduct of the study, and grants and personal fees from Boehringer Ingelheim, grants and personal fees from Roche, and personal fees from Galapagos outside the submitted work; MK reports grants from Roche during the conduct of the study, and personal fees from Roche and Boehringer Ingelheim outside the submitted work; CH, SET and CG has nothing to disclose.
Figures

References
-
- Travis WD, Costabel U, Hansell DM, King TE, Lynch DA, Nicholson AG, et al. An Official American Thoracic Society/European Respiratory Society Statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188:733–748. doi: 10.1164/rccm.201308-1483ST. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
