

SARS-CoV-2 positivity in offspring and timing of mother-to-child transmission: living systematic review and meta-analysis
- PMID: 35296519
- PMCID: PMC8924705
- DOI: 10.1136/bmj-2021-067696
SARS-CoV-2 positivity in offspring and timing of mother-to-child transmission: living systematic review and meta-analysis
Abstract
Objectives: To assess the rates of SARS-CoV-2 positivity in babies born to mothers with SARS-CoV-2 infection, the timing of mother-to-child transmission and perinatal outcomes, and factors associated with SARS-CoV-2 status in offspring.
Design: Living systematic review and meta-analysis.
Data sources: Major databases between 1 December 2019 and 3 August 2021.
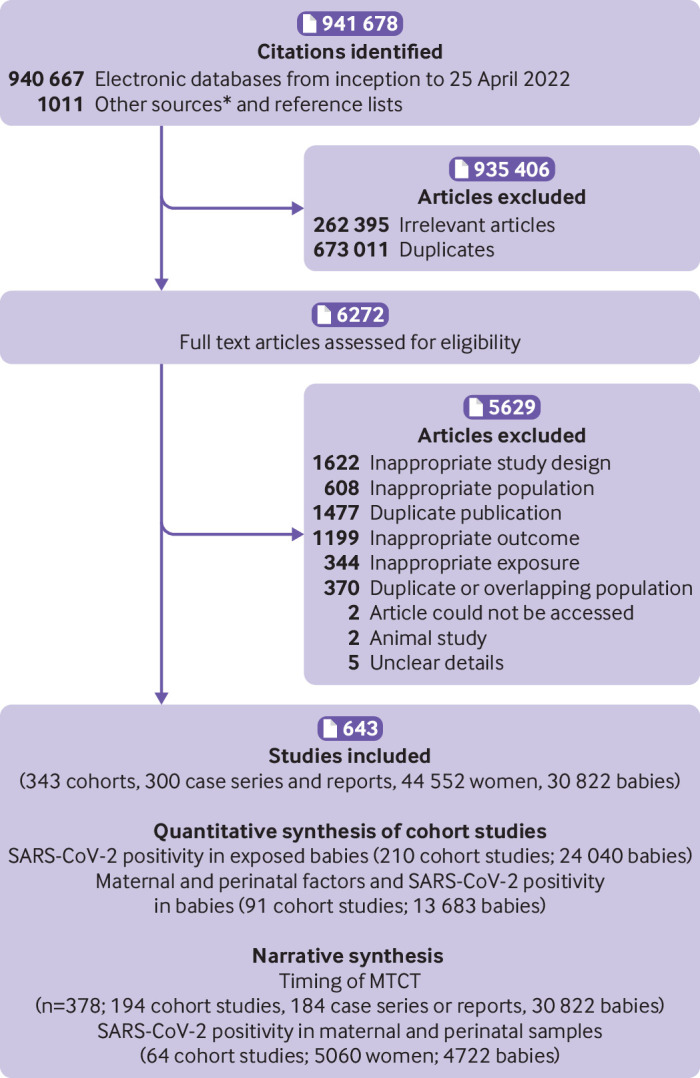
Study selection: Cohort studies of pregnant and recently pregnant women (including after abortion or miscarriage) who sought hospital care for any reason and had a diagnosis of SARS-CoV-2 infection, and also provided data on offspring SARS-CoV-2 status and risk factors for positivity. Case series and case reports were also included to assess the timing and likelihood of mother-to-child transmission in SARS-CoV-2 positive babies.
Data extraction: Two reviewers independently extracted data and assessed study quality. A random effects model was used to synthesise data for rates, with associations reported using odds ratios and 95% confidence intervals. Narrative syntheses were performed when meta-analysis was inappropriate. The World Health Organization classification was used to categorise the timing of mother-to-child transmission (in utero, intrapartum, early postnatal).
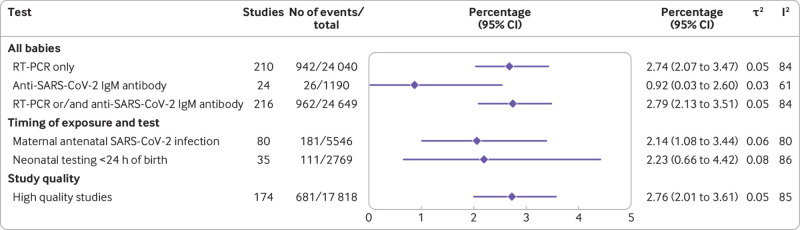
Results: 472 studies (206 cohort studies, 266 case series and case reports; 28 952 mothers, 18 237 babies) were included. Overall, 1.8% (95% confidence interval 1.2% to 2.5%; 140 studies) of the 14 271 babies born to mothers with SARS-CoV-2 infection tested positive for the virus with reverse transcriptase polymerase chain reaction (RT-PCR). Of the 592 SARS-CoV-2 positive babies with data on the timing of exposure and type and timing of tests, 14 had confirmed mother-to-child transmission: seven in utero (448 assessed), two intrapartum (18 assessed), and five during the early postnatal period (70 assessed). Of the 800 SARS-CoV-2 positive babies with outcome data, 20 were stillbirths, 23 were neonatal deaths, and eight were early pregnancy losses; 749 babies were alive at the end of follow-up. Severe maternal covid-19 (odds ratio 2.4, 95% confidence interval 1.3 to 4.4), maternal death (14.1, 4.1 to 48.0), maternal admission to an intensive care unit (3.5, 1.7 to 6.9), and maternal postnatal infection (5.0, 1.2 to 20.1) were associated with SARS-CoV-2 positivity in offspring. Positivity rates using RT-PCR varied between regions, ranging from 0.1% (95% confidence interval 0.0% to 0.3%) in studies from North America to 5.7% (3.2% to 8.7%) in studies from Latin America and the Caribbean.
Conclusion: SARS-CoV-2 positivity rates were found to be low in babies born to mothers with SARS-CoV-2 infection. Evidence suggests confirmed vertical transmission of SARS-CoV-2, although this is likely to be rare. Severity of maternal covid-19 appears to be associated with SARS-CoV-2 positivity in offspring.
Systematic review registration: PROSPERO CRD42020178076.
Readers' note: This article is a living systematic review that will be updated to reflect emerging evidence. Updates may occur for up to two years from the date of original publication.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: partial funding by the World Health Organization and the UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
Figures

Comment in
-
Transmission of SARS-CoV-2 from mother to baby is rare.BMJ. 2022 Mar 16;376:o593. doi: 10.1136/bmj.o593. BMJ. 2022. PMID: 35296505 No abstract available.
-
Update to living systematic review on SARS-CoV-2 positivity in offspring and timing of mother-to-child transmission.BMJ. 2024 Jan 10;384:2929. doi: 10.1136/bmj.p2929. BMJ. 2024. PMID: 38199645 No abstract available.
References
-
- Breslin N, Baptiste C, Gyamfi-Bannerman C, et al. Coronavirus disease 2019 infection among asymptomatic and symptomatic pregnant women: two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am J Obstet Gynecol MFM 2020;2:100118. 10.1016/j.ajogmf.2020.100118 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous