

The arterialised saphenous venous flow-through flap for managing the radial forearm free flap donor site
- PMID: 35297112
- PMCID: PMC9315149
- DOI: 10.1002/micr.30883
The arterialised saphenous venous flow-through flap for managing the radial forearm free flap donor site
Abstract
Background: The radial forearm fasciocutaneous flap (RFFF) is a workhorse flap, however concerns with donor site morbidity include tendon exposure, delayed wound healing, impaired sensitivity, and poor cosmesis, have seen it fall out of favor. We present a method of using an arterialised saphenous flow through flap to reconstruct the RFFF donor site.
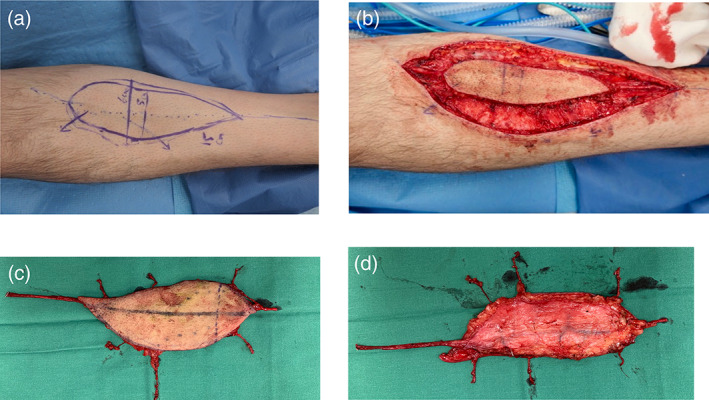
Method: A cohort study of six patients (five male, one female; mean age 59 [range 19-90]) who had their RFFF donor site reconstructed with an arterialised saphenous flow through flap is presented. The use of multiple peripheral efferent venous anastomoses, flap rotation 180 degrees prior to inset, and the ligation of intra-flap connecting veins were three modifications employed. Primary outcomes include complication rates. Secondary outcomes were patient reported outcome measures via the Michigan Hand Outcomes Questionnaire, and patency and flow through the flap.
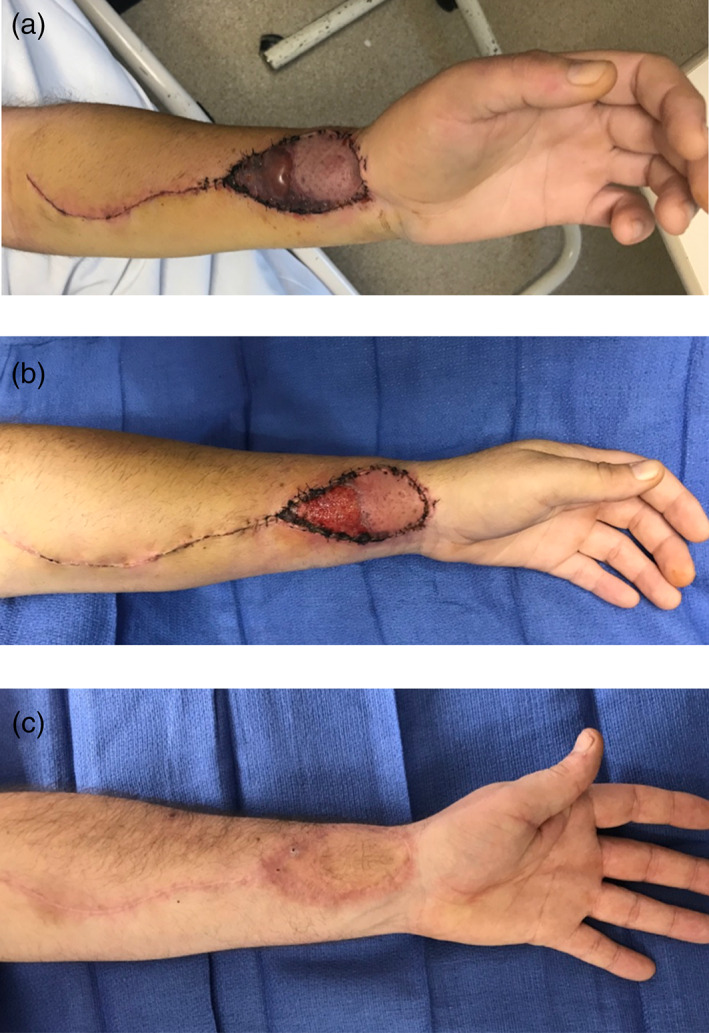
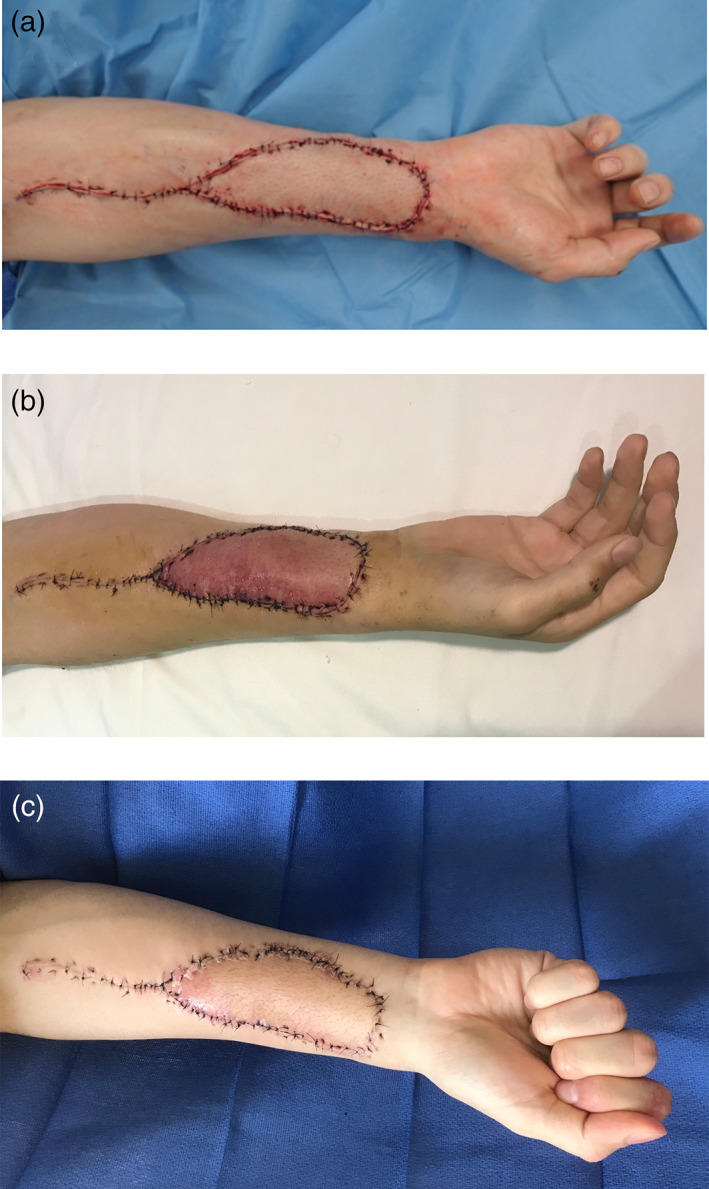
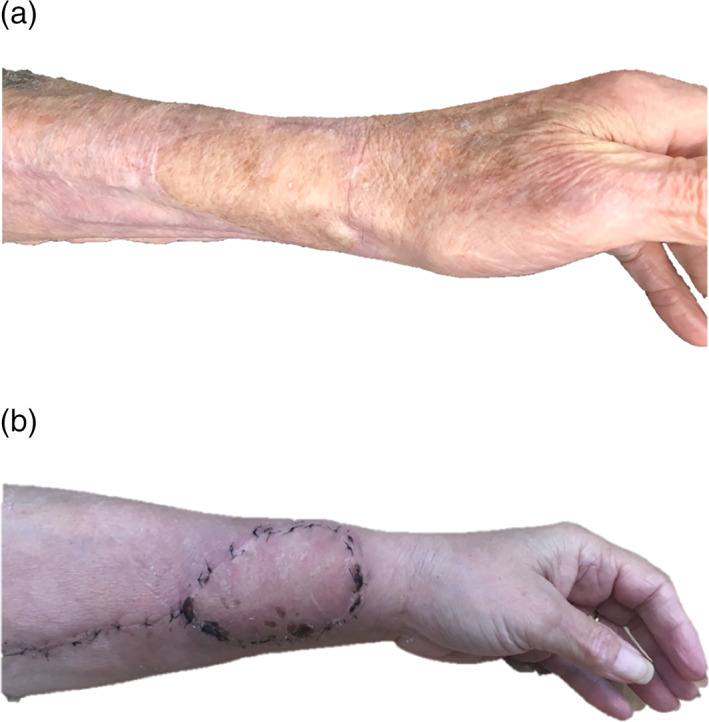
Results: In all six cases, there was flap survival. RFFF dimensions ranging from lengths of 6-15 cm (mean 11.5 cm) and widths of 4-6 cm (mean 5.3 cm), with an average flap area of 58 cm2 (range 24-90). There were no total flap losses, one partial superficial flap loss and one minor donor site delayed healing, over a mean follow-up of 6 months (4-24 months). The average overall patient satisfaction was 91 on Michigan Hand Outcomes Questionnaire. Pain was well tolerated with a low average pain score of 15.
Conclusion: The modified arterialised saphenous flow through flap is a useful option for reconstructing the soft tissue defect and reconstituting the radial artery after RFFF harvest.
© 2022 The Authors. Microsurgery published by Wiley Periodicals LLC.
Conflict of interest statement
There are no conflicts of interest for any of the authors or affiliations, and the authors declare no knowledge of any direct interest, particularly a financial interest, in the subject matter or materials discussed. The authors have no employment by an industrial concern, ownership of stock, membership on a standing advisory council or committee, a seat on the board of directors, or being publicly associated with a company or its products that may pose such an interest. The authors have no real or perceived conflict of interest that include receiving honoraria or consulting fees or receiving grants or funds from such corporations or individuals representing such corporations. There was no grant, research scholarship or financial support provided for the study. There is no conflict of interest on preparation of this manuscript.
Figures

Similar articles
-
The radial forearm snake flap: An underutilized technique for fasciocutaneous and osteocutaneous forearm flaps with primary closure.Head Neck. 2022 May;44(5):1106-1113. doi: 10.1002/hed.27004. Epub 2022 Feb 14. Head Neck. 2022. PMID: 35165977
-
Coverage of radial forearm free flap donor site defect using another free flap.Microsurgery. 2023 Nov;43(8):775-781. doi: 10.1002/micr.31082. Epub 2023 Jul 6. Microsurgery. 2023. PMID: 37415398
-
Full-thickness skin graft versus split-thickness skin graft for radial forearm free flap donor site closure: protocol for a systematic review and meta-analysis.Syst Rev. 2024 Feb 26;13(1):74. doi: 10.1186/s13643-024-02471-x. Syst Rev. 2024. PMID: 38409059 Free PMC article.
-
Comparing donor site morbidity between radial and ulnar forearm free flaps: a meta-analysis.Br J Oral Maxillofac Surg. 2022 Jun;60(5):547-553. doi: 10.1016/j.bjoms.2021.10.014. Epub 2021 Nov 9. Br J Oral Maxillofac Surg. 2022. PMID: 35437195 Review.
-
Is there an ideal way to close the donor site of radial forearm free flaps?Br J Oral Maxillofac Surg. 2018 Jul;56(6):444-452. doi: 10.1016/j.bjoms.2018.04.016. Epub 2018 May 30. Br J Oral Maxillofac Surg. 2018. PMID: 29859780 Review.
References
-
- Bonaparte, J. P. , Corsten, M. J. , Odell, M. , Gupta, M. , Allen, M. , & Tse, D. (2013). Management of the radial forearm free flap donor site using a topically applied tissue expansion device. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, 116(1), 28–34. 10.1016/j.oooo.2013.01.007 - DOI - PubMed
-
- De Lorenzi, F. , van der Hulst, R. R. , den Dunnen, W. F. , Vranckx, J. J. , Vandenhof, B. , Francois, C. , & Boeckx, W. D. (2002). Arterialized venous free flaps for soft‐tissue reconstruction of digits: A 40‐case series. Journal of Reconstructive Microsurgery, 18(7), 569–574. 10.1055/s-2002-35093 - DOI - PubMed
-
- Hamahata, A. , Beppu, T. , Osada, A. , Yamaki, T. , & Sakurai, H. (2016). An alternative method of the direct closure for the radial forearm flap donor‐site defect: Lazy S double‐opposing rotation flaps. Journal of Reconstructive Microsurgery Open, 1(1), 63–66. 10.1055/s-0036-1580607 - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
