

Understanding shoulder pseudoparalysis: Part I: Definition to diagnosis
- PMID: 35298415
- PMCID: PMC8965199
- DOI: 10.1530/EOR-21-0069
Understanding shoulder pseudoparalysis: Part I: Definition to diagnosis
Abstract
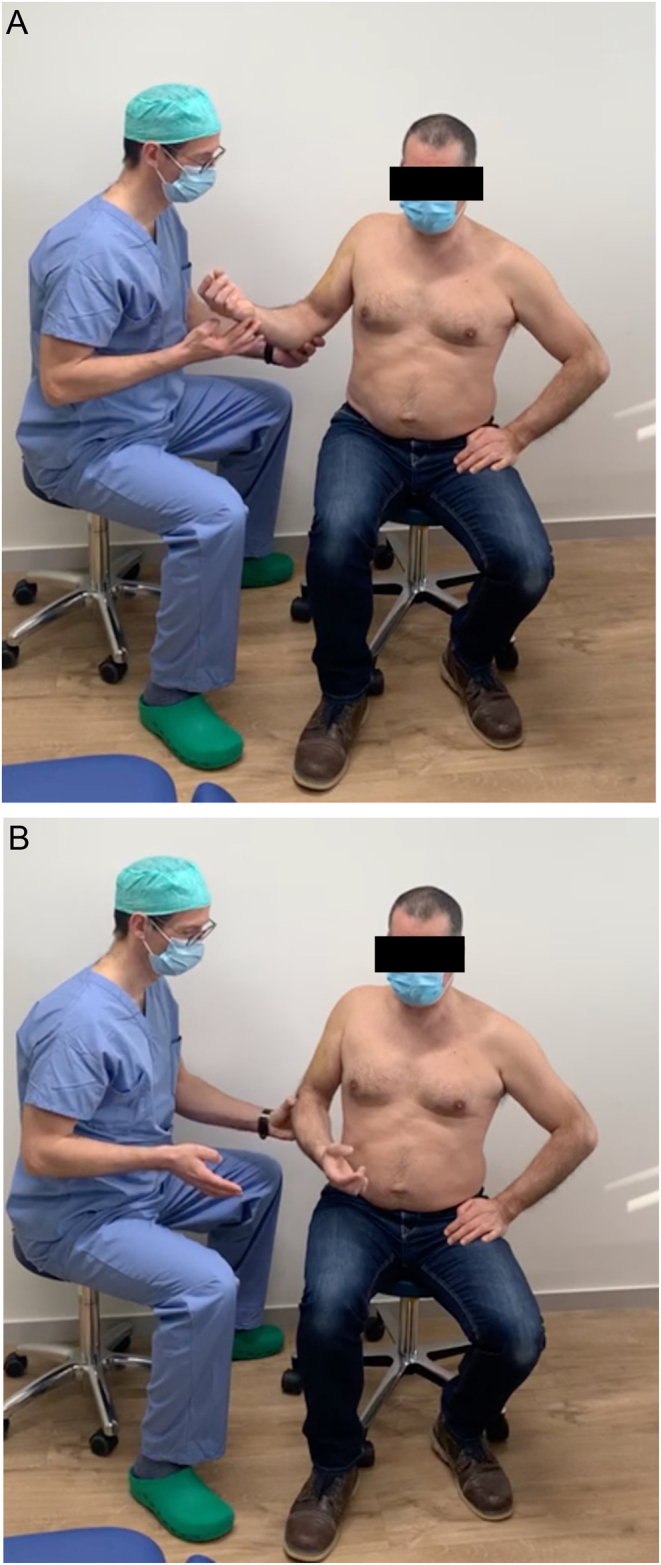
Variable definitions of pseudoparalysis have been used in the literature. Recent systematic reviews and biomechanical studies call for a grading of loss of force couple balance and the use of the terms 'pseudoparesis' and 'pseudoparalysis'. Pain should be excluded as the cause of loss of active function. Key players for loss of force couple balance seem to be the lower subscapularis as an anterior inferior checkrein and the teres minor as a posterior inferior fulcrum. Loss of three out of five muscle-tendon units counting upper and lower subscapularis separately is predictive of pseudoparalysis. Shoulder equator concept: loss of all three posterior, or all three superior, or all three anterior muscle-tendon units is predictive of pseudoparalysis (loss of fulcrum for deltoid force). Every effort should be made to prevent propagation of rotator cuff tears into the subscapularis and posterior rotator cuff (infraspinatus and teres minor) to maintain force couple balance (value of partial cuff repair). Clinical assessment of active forward elevation, active external rotation, and active internal rotation is important to define and grade the severity of loss of force couple balance. Additional features such as patient age, traumatic aetiology, chronicity, fatty infiltration, and stage of cuff tear arthropathy are useful for a specific diagnosis with implications for treatment.
Keywords: arthroscopy; pseudoparalysis; shoulder.
Figures









References
-
- Werner CM, Steinmann PA, Gilbart M, Gerber C. Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the delta III reverse-ball-and-socket total shoulder prosthesis. Journal of Bone and Joint Surgery: American Volume 2005. 87 1476–1486. ( 10.2106/JBJS.D.02342) - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
