

Association between lithium use and the incidence of dementia and its subtypes: A retrospective cohort study
- PMID: 35298477
- PMCID: PMC8929585
- DOI: 10.1371/journal.pmed.1003941
Association between lithium use and the incidence of dementia and its subtypes: A retrospective cohort study
Abstract
Background: Dementia is the leading cause of death in elderly Western populations. Preventative interventions that could delay dementia onset even modestly would provide a major public health impact. There are no disease-modifying treatments currently available. Lithium has been proposed as a potential treatment. We assessed the association between lithium use and the incidence of dementia and its subtypes.
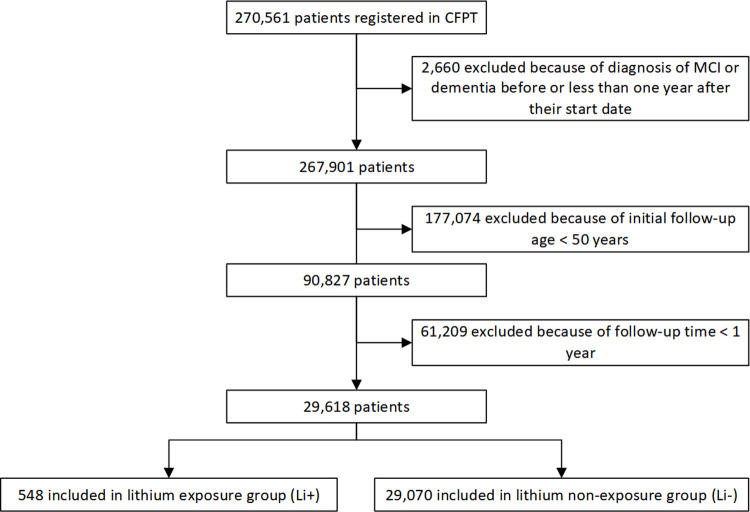
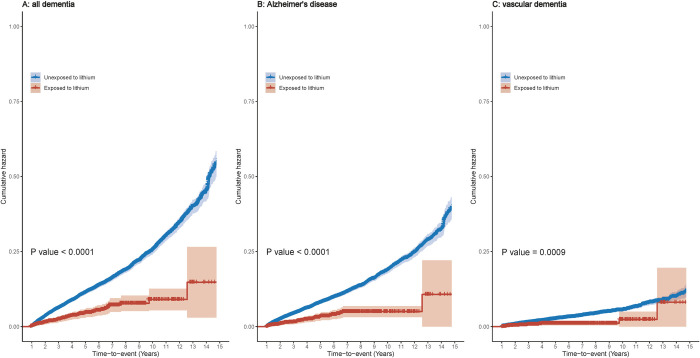
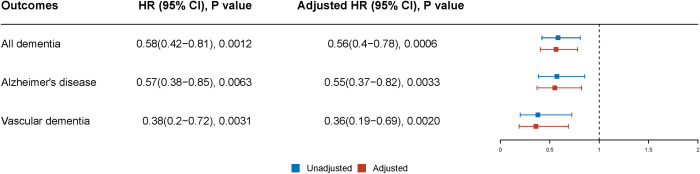
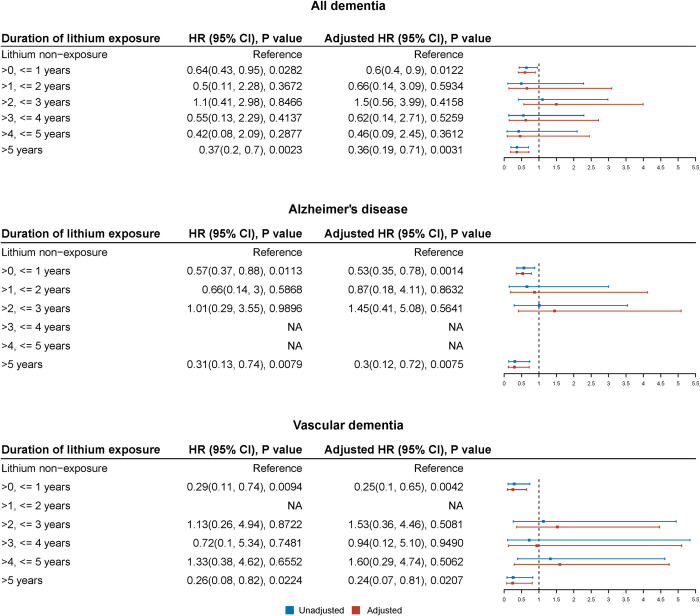
Methods and findings: We conducted a retrospective cohort study comparing patients treated between January 1, 2005 and December 31, 2019, using data from electronic clinical records of secondary care mental health (MH) services in Cambridgeshire and Peterborough NHS Foundation Trust (CPFT), United Kingdom (catchment area population approximately 0.86 million). Eligible patients were those aged 50 years or over at baseline and who had at least 1 year follow-up, excluding patients with a diagnosis of mild cognitive impairment (MCI) or dementia before, or less than 1 year after, their start date. The intervention was the use of lithium. The main outcomes were dementia and its subtypes, diagnosed and classified according to the International Classification of Diseases-10th Revision (ICD-10). In this cohort, 29,618 patients (of whom 548 were exposed to lithium) were included. Their mean age was 73.9 years. A total of 40.2% were male, 33.3% were married or in a civil partnership, and 71.0% were of white ethnicity. Lithium-exposed patients were more likely to be married, cohabiting or in a civil partnership, to be a current/former smoker, to have used antipsychotics, and to have comorbid depression, mania/bipolar affective disorder (BPAD), hypertension, central vascular disease, diabetes mellitus, or hyperlipidemias. No significant difference between the 2 groups was observed for other characteristics, including age, sex, and alcohol-related disorders. In the exposed cohort, 53 (9.7%) patients were diagnosed with dementia, including 36 (6.8%) with Alzheimer disease (AD) and 13 (2.6%) with vascular dementia (VD). In the unexposed cohort, corresponding numbers were the following: dementia 3,244 (11.2%), AD 2,276 (8.1%), and VD 698 (2.6%). After controlling for sociodemographic factors, smoking status, other medications, other mental comorbidities, and physical comorbidities, lithium use was associated with a lower risk of dementia (hazard ratio [HR] 0.56, 95% confidence interval [CI] 0.40 to 0.78), including AD (HR 0.55, 95% CI 0.37 to 0.82) and VD (HR 0.36, 95% CI 0.19 to 0.69). Lithium appeared protective in short-term (≤1-year exposure) and long-term lithium users (>5-year exposure); a lack of difference for intermediate durations was likely due to lack of power, but there was some evidence for additional benefit with longer exposure durations. The main limitation was the handling of BPAD, the most common reason for lithium prescription but also a risk factor for dementia. This potential confounder would most likely cause an increase in dementia in the exposed group, whereas we found the opposite, and the sensitivity analysis confirmed the primary results. However, the specific nature of the group of patients exposed to lithium means that caution is needed in extending these findings to the general population. Another limitation is that our sample size of patients using lithium was small, reflected in the wide CIs for results relating to some durations of lithium exposure, although again sensitivity analyses remained consistent with our primary findings.
Conclusions: We observed an association between lithium use and a decreased risk of developing dementia. This lends further support to the idea that lithium may be a disease-modifying treatment for dementia and that this is a promising treatment to take forwards to larger randomised controlled trials (RCTs) for this indication.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: SC, and JRL declare no conflict of interest with this work. PBJ is a scientific advisory board member for Janssen and Recordati. BRU is clinical director for older people’s and adult community services at CPFT. He is clinical director of the Windsor Unit at Fulbourn Hospital (CPFT), which delivers clinical trials in dementia/mild cognitive impairment for academic and commercial organisations without personal benefit, and is the clinical lead for dementia for the NIHR Clinical Research Network (CRN) in the East of England. His salary is part-funded by the NIHR CRN. His lectureship is funded by Gnodde Goldman-Sachs Giving. He has been principal investigator on trials for Axovant, Lilly, and EIP Pharma; his institution has benefited from payment for research carried out but he has not personally received any money. His wife is the lead for mental health for Suffolk Clinical Commissioning Group. RNC consults for Campden Instruments Ltd and receives royalties from Cambridge University Press, Cambridge Enterprise, and Routledge.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
