

Vascular complications after liver transplantation: a 5-year experience
- PMID: 3529892
- PMCID: PMC3095891
- DOI: 10.2214/ajr.147.4.657
Vascular complications after liver transplantation: a 5-year experience
Abstract
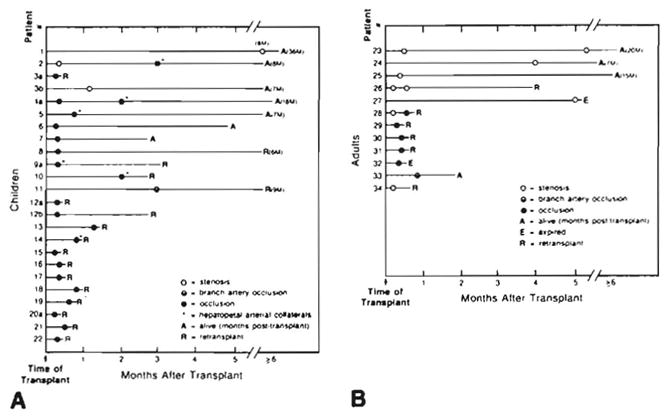
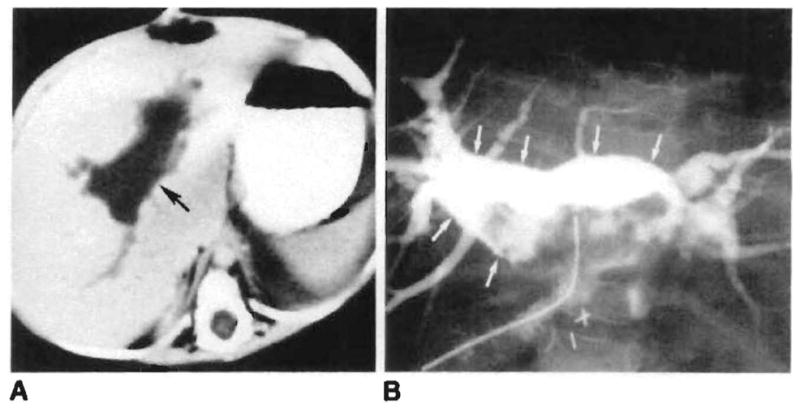
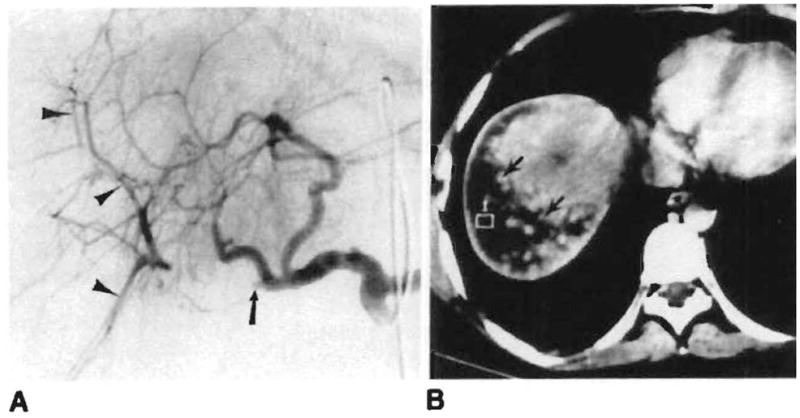
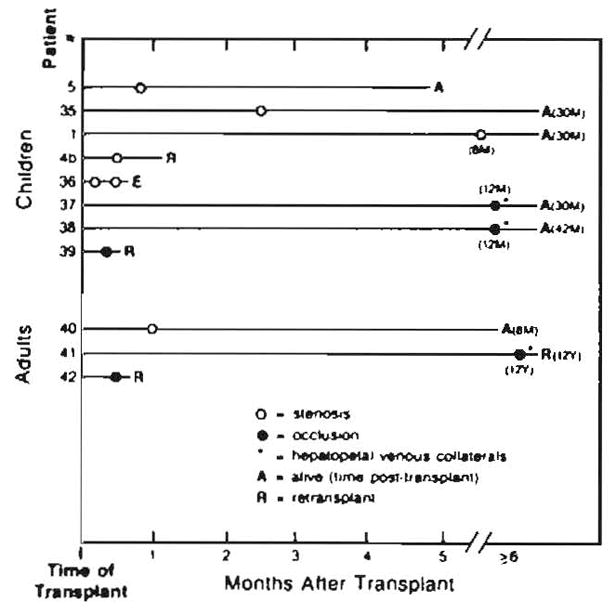
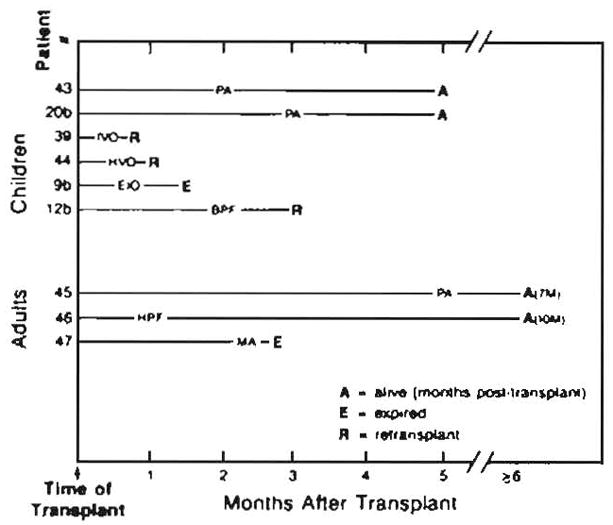
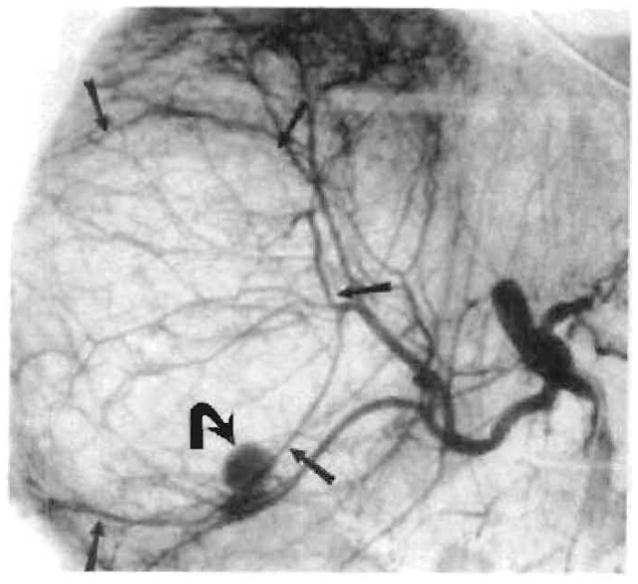
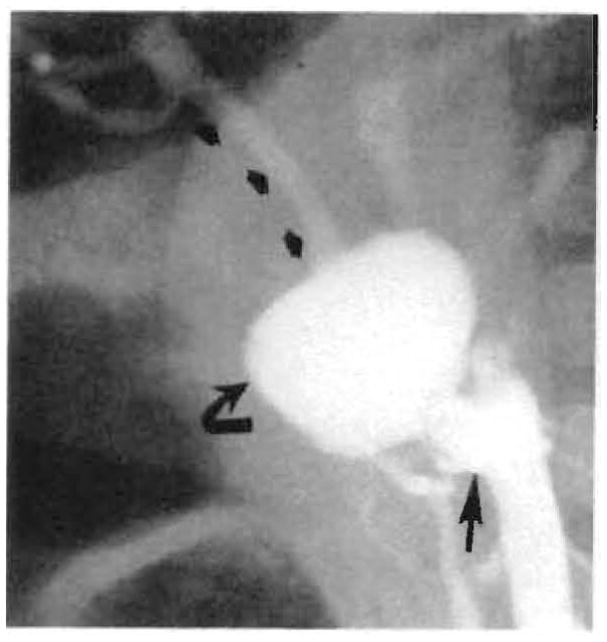
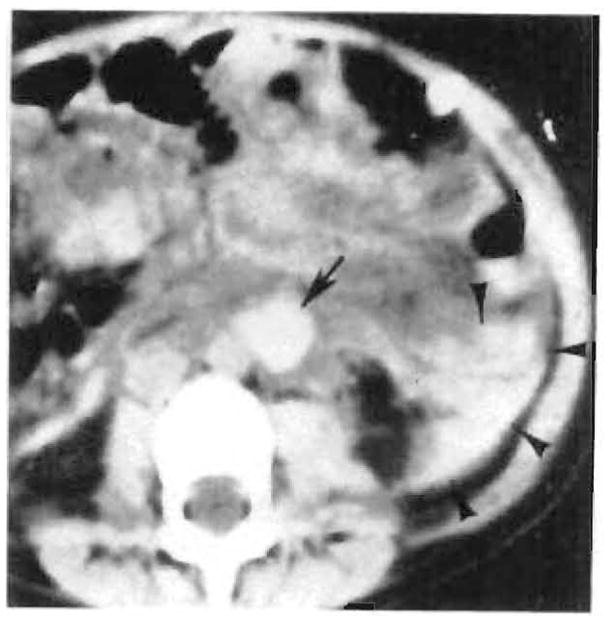
During the past 5 years, 104 angiographic studies were performed in 87 patients (45 children and 42 adults) with 92 transplanted livers for evaluation of possible vascular complications. Seventy percent of the studies were abnormal. Hepatic artery thrombosis was the most common complication (seen in 42% of children studied, compared with only 12% of adults) and was a major complication that frequently resulted in graft failure, usually necessitating retransplantation. In six children, reconstitution of the intrahepatic arteries by collaterals was seen. Three survived without retransplant. Arterial stenosis at the anastomosis or in the donor hepatic artery was observed in 11% of patients. Portal vein thrombosis or stenosis occurred in 13% of patients. Two children and one adult with portal vein thrombosis demonstrated hepatopetal collaterals that reconstituted the intrahepatic portal vessels. Uncommon complications included anastomotic and donor hepatic artery pseudoaneurysms, a hepatic artery-dissecting aneurysm, pancreaticoduodenal mycotic aneurysms, hepatic artery-portal vein fistula, biliary-portal vein fistula, hepatic vein occlusion, and inferior vena cava thrombosis.
Figures

References
-
- Starzl TE, Iwatsuki S, Shaw BW, Jr, Gordon RD. Orthotopic liver transplantation in 1984. Transplant Proc. 1985;17:250–258.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
