

The PRIMARY Score: Using Intraprostatic 68Ga-PSMA PET/CT Patterns to Optimize Prostate Cancer Diagnosis
- PMID: 35301240
- PMCID: PMC9635676
- DOI: 10.2967/jnumed.121.263448
The PRIMARY Score: Using Intraprostatic 68Ga-PSMA PET/CT Patterns to Optimize Prostate Cancer Diagnosis
Abstract
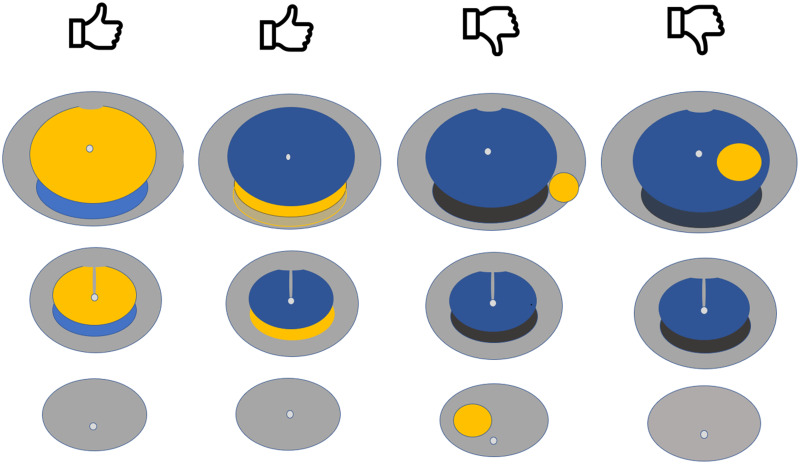
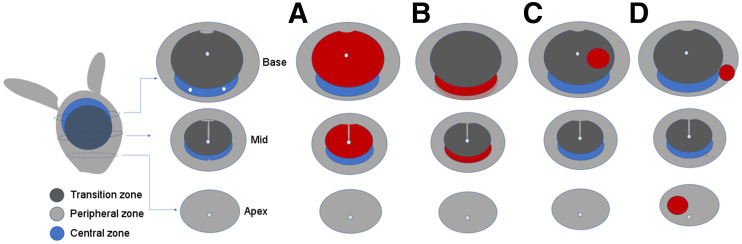
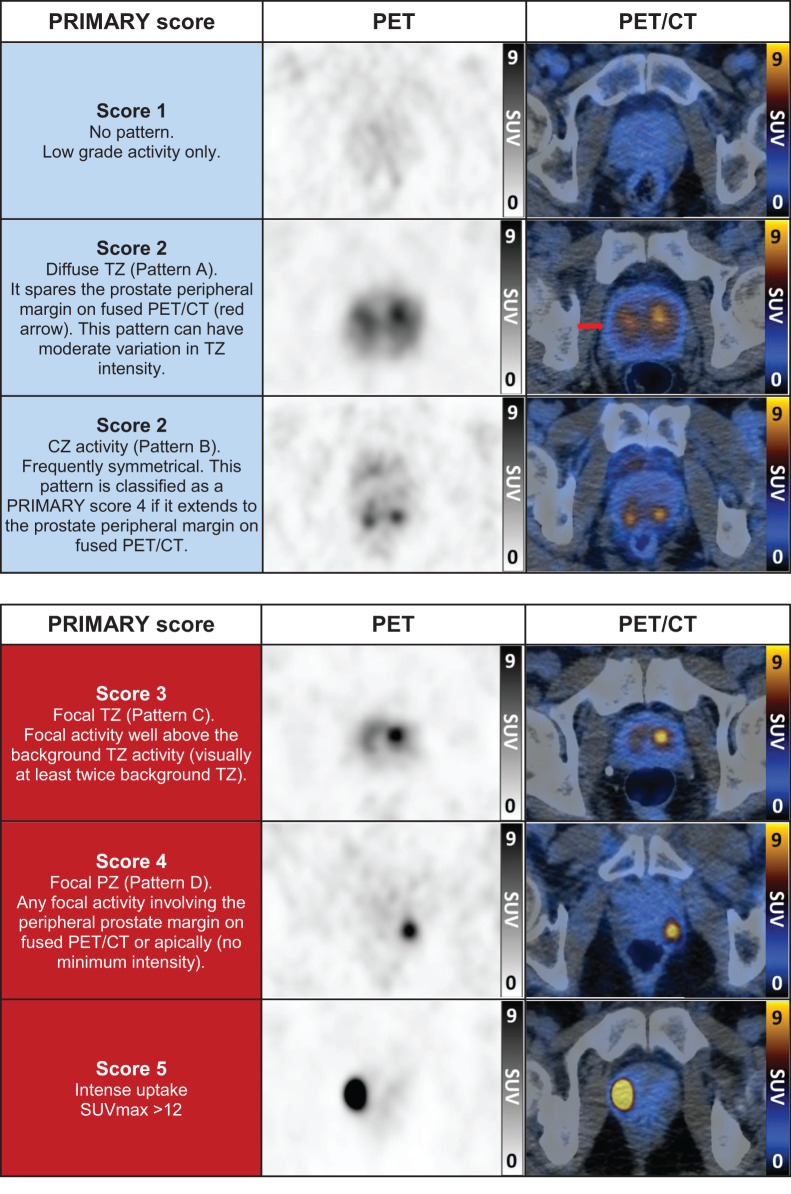
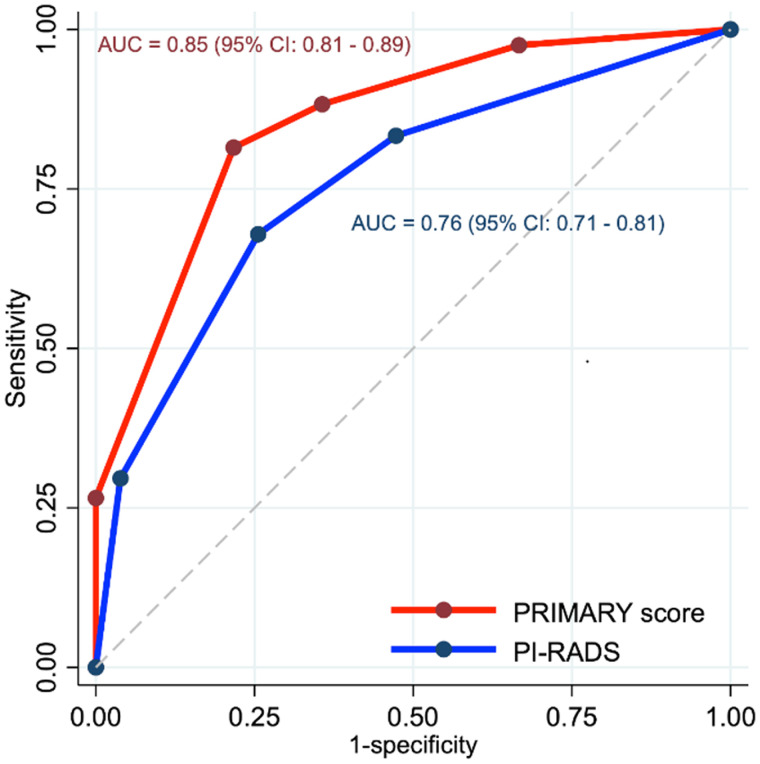
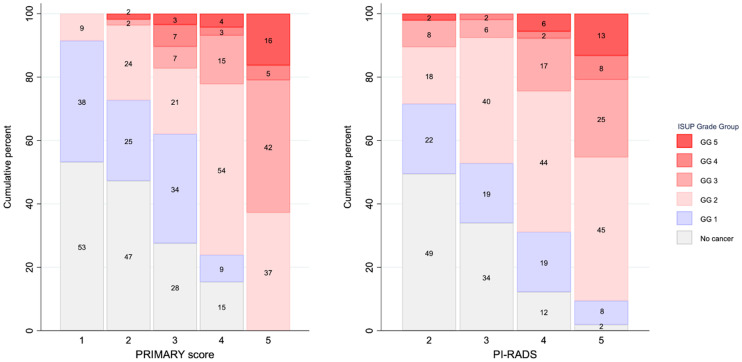
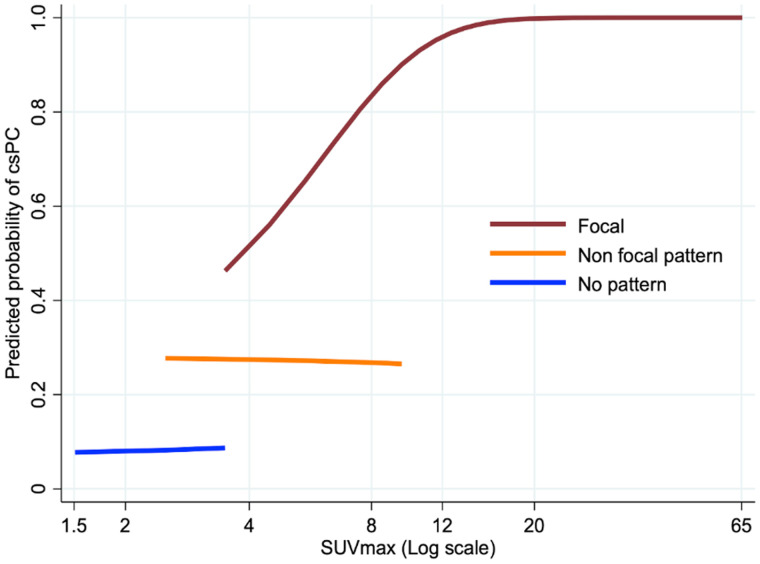
Multiparametric MRI (mpMRI) is validated for the diagnosis of clinically significant prostate cancer (csPCa). 68Ga-PSMA-11 PET/CT (68Ga-PSMA PET/CT) combined with mpMRI has improved negative predictive value over mpMRI alone for csPCa. The aim of this post hoc analysis of the PRIMARY study was to evaluate the clinical significance of patterns of intraprostatic PSMA activity, proposing a 5-point PRIMARY score to optimize the accuracy of 68Ga-PSMA PET/CT for csPCa in a low-prevalence population. Methods: The PRIMARY trial was a prospective multicenter phase II imaging trial that enrolled men with suspected PCa, no prior biopsy, and a recent mpMRI examination (6 mo) and for whom prostate biopsy was planned. In total, 291 men underwent mpMRI, 68Ga-PSMA PET/CT, and systematic biopsy with or without targeted biopsy. The mpMRI was read separately using the Prostate Imaging Reporting and Data System (PI-RADS) (version 2). 68Ga-PSMA PET/CT (pelvis only) was acquired a minimum of 60 min after injection. 68Ga-PSMA PET/CT was centrally read for pattern (diffuse transition zone [TZ], symmetric central zone [CZ], focal TZ, or focal peripheral zone [PZ]) and intensity (SUVmax). In this post hoc analysis, a 5-level PRIMARY score was assigned on the basis of analysis of the central read: no pattern (score of 1), diffuse TZ or CZ (not focal) (score of 2), focal TZ (score of 3), focal PZ (score of 4), or an SUVmax of at least 12 (score of 5). Two further readers independently assigned a PRIMARY score to 118 scans to determine interrater agreement. Associations between PRIMARY score and csPCa (International Society of Urological Pathology grade group ≥ 2) were evaluated. Results: Of the 291 men enrolled, 162 (56%) had csPCa. A PRIMARY score of 1 was present in 16% (47); a score of 2, in 19% (55); a score of 3, in 10% (29); a score of 4 in 40% (117); and a score of 5, in 15% (43). The proportion of patients with csPCa and a PRIMARY score of 1, 2, 3, 4, and 5 was 8.5% (4/47), 27% (15/55), 38% (11/29), 76% (89/117), and 100% (43/43), respectively. Sensitivity, specificity, positive predictive value, and negative predictive value for a PRIMARY score of 1 or 2 (low-risk patterns) versus a PRIMARY score of 3-5 (high-risk patterns) were 88%, 64%, 76%, and 81%, respectively, compared with 83%, 53%, 69%, and 72%, respectively, for a PI-RADS score of 2 versus 3-5 on mpMRI. The Cohen κ for a PRIMARY score of 1 of 2 versus a PRIMARY score of 3-5 was 0.76 (95% CI, 0.64-0.88) for reader 1 and 0.64 (95% CI, 0.49-0.78) for reader 2. Conclusion: A PRIMARY score incorporating intraprostatic pattern and intensity on 68Ga-PSMA PET/CT shows potential, with high diagnostic accuracy for csPCa. Further validation is warranted before implementation.
Keywords: PET; PSMA; diagnosis; multiparametric MRI; prostate cancer; prostate-specific membrane antigen.
© 2022 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
-
- Turkbey B, Rosenkrantz AB, Haider MA, et al. . Prostate imaging reporting and data system version 2.1: 2019 update of prostate imaging reporting and data system version 2. Eur Urol. 2019;76:340–351. - PubMed
-
- Emmett L, Buteau J, Papa N, et al. . The additive diagnostic value of prostate-specific membrane antigen positron emission tomography computed tomography to multiparametric magnetic resonance imaging triage in the diagnosis of prostate cancer (PRIMARY): a prospective multicentre study. Eur Urol. 2021;80:682–689. - PubMed
-
- Eiber M, Nekolla SG, Maurer T, Weirich G, Wester HJ, Schwaiger M. 68Ga-PSMA PET/MR with multimodality image analysis for primary prostate cancer. Abdom Imaging. 2015;40:1769–1771. - PubMed
-
- Scheltema MJ, Chang JI, Stricker PD, et al. . Diagnostic accuracy of 68Ga-prostate-specific membrane antigen (PSMA) positron-emission tomography (PET) and multiparametric (mp)MRI to detect intermediate-grade intra-prostatic prostate cancer using whole-mount pathology: impact of the addition of 68Ga-PSMA PET to mpMRI. BJU Int. 2019;124(suppl 1):42–49. - PubMed
-
- Amin A, Blazevski A, Thompson J, et al. . Protocol for the PRIMARY clinical trial, a prospective, multicentre, cross-sectional study of the additive diagnostic value of gallium-68 prostate-specific membrane antigen positron-emission tomography/computed tomography to multiparametric magnetic resonance imaging in the diagnostic setting for men being investigated for prostate cancer. BJU Int. 2020;125:515–524. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous