

De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: a case report
- PMID: 35301314
- PMCID: PMC8930970
- DOI: 10.1038/s41467-022-29104-y
De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: a case report
Abstract
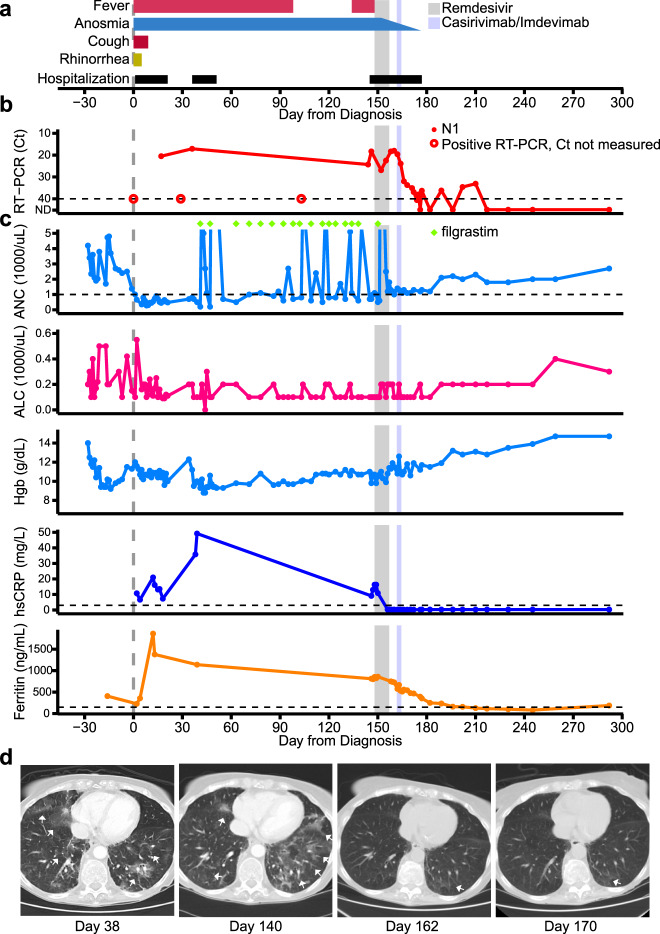
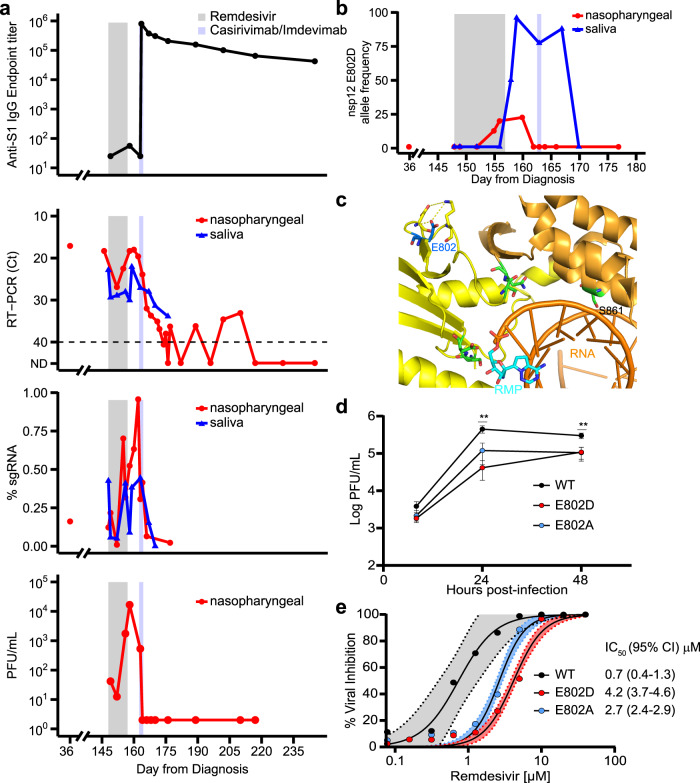
SARS-CoV-2 remdesivir resistance mutations have been generated in vitro but have not been reported in patients receiving treatment with the antiviral agent. We present a case of an immunocompromised patient with acquired B-cell deficiency who developed an indolent, protracted course of SARS-CoV-2 infection. Remdesivir therapy alleviated symptoms and produced a transient virologic response, but her course was complicated by recrudescence of high-grade viral shedding. Whole genome sequencing identified a mutation, E802D, in the nsp12 RNA-dependent RNA polymerase, which was not present in pre-treatment specimens. In vitro experiments demonstrated that the mutation conferred a ~6-fold increase in remdesivir IC50 but resulted in a fitness cost in the absence of remdesivir. Sustained clinical and virologic response was achieved after treatment with casirivimab-imdevimab. Although the fitness cost observed in vitro may limit the risk posed by E802D, this case illustrates the importance of monitoring for remdesivir resistance and the potential benefit of combinatorial therapies in immunocompromised patients with SARS-CoV-2 infection.
© 2022. The Author(s).
Conflict of interest statement
A.L.G. reports institutional central testing contracts from Abbott and research grants from Merck and Gilead, outside of the proposed work. A.I.K. received consulting fees from Tata Sons and is the recipient of grants on COVID-19 from Merck, Regeneron and Serimmune, all of which are outside the submitted work. O.O. received consulting fees from Gilead and ViiV, as well as research support and honoraria from Gilead, outside of the submitted work. W.L.S. is a consultant for Hugo Health, founder of Refactor Health and is recipient of grants on COVID-19 from Merck and Regeneron, all of which are outside the submitted work. The remaining authors declare no competing interests.
Figures
Update of
-
De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: A case report.medRxiv [Preprint]. 2021 Dec 7:2021.11.08.21266069. doi: 10.1101/2021.11.08.21266069. medRxiv. 2021. Update in: Nat Commun. 2022 Mar 17;13(1):1547. doi: 10.1038/s41467-022-29104-y. PMID: 34909781 Free PMC article. Updated. Preprint.
References
-
- Collaboration, T. C.-N. B. C.-19 et al. SARS-CoV-2 evolution during treatment of chronic infection. Nature 1–10 10.1038/s41586-021-03291-y (2021).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
