

Cardiac sympathetic denervation in the prevention of genetically mediated life-threatening ventricular arrhythmias
- PMID: 35301528
- PMCID: PMC9459868
- DOI: 10.1093/eurheartj/ehac134
Cardiac sympathetic denervation in the prevention of genetically mediated life-threatening ventricular arrhythmias
Erratum in
-
Corrigendum to: Cardiac sympathetic denervation in the prevention of genetically mediated life-threatening ventricular arrhythmias.Eur Heart J. 2022 Sep 1;43(33):3181. doi: 10.1093/eurheartj/ehac380. Eur Heart J. 2022. PMID: 35801806 Free PMC article. No abstract available.
Abstract
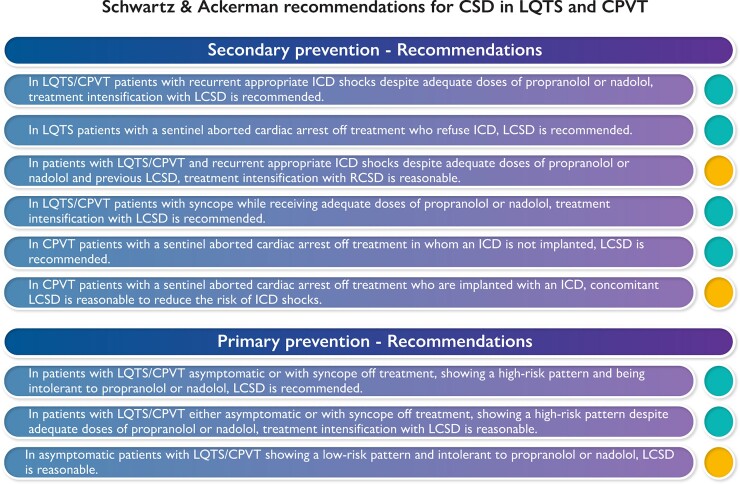
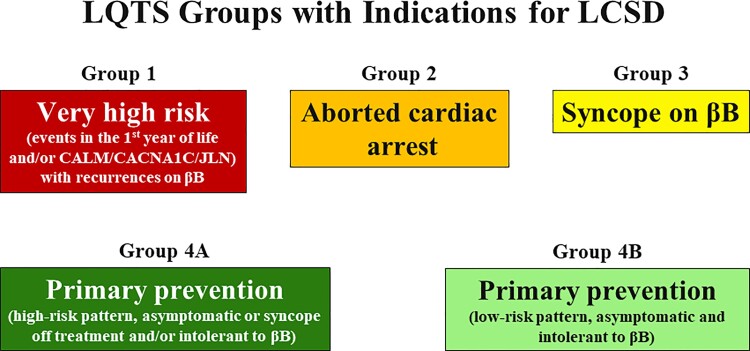
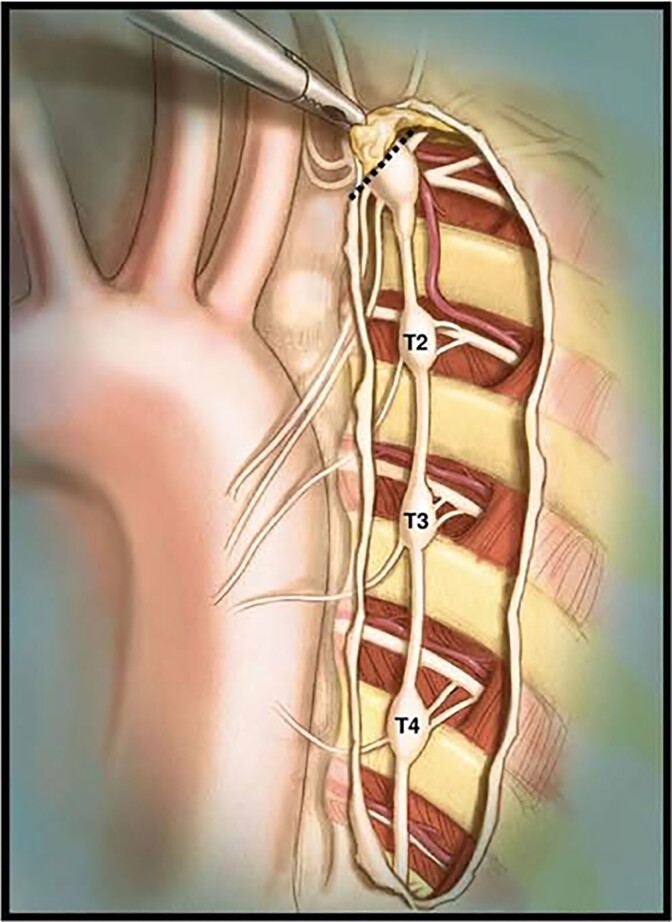
Proper management of patients affected by genetic disorders causing life-threatening arrhythmias is important for several reasons, including even societal ones, given the predominantly young age of those affected. Incorrect management often has dire consequences, ranging from unnecessary psychologic damage for the patients whose life becomes too limited by the fear of sudden death to equally avoidable tragedies when the entire armamentarium of effective therapies is not fully utilized. In this review, we focus primarily on long QT syndrome (LQTS) and catecholaminergic polymorphic ventricular tachycardia (CPVT) and deal specifically with the clinical impact of the most commonly used cardiac sympathetic denervation (CSD), namely left cardiac sympathetic denervation (LCSD). The two of us have used LCSD in the management of our patients with either LQTS or CPVT for a very long time and have been involved in ∼500 such interventions. It is on the basis of this personal and direct experience that we wish to share our views with clinical cardiologists and electrophysiologists, adult and paediatric, and with genetic cardiologists. We will begin by reviewing the history and rationale underlying sympathetic denervation therapy and will continue with a disease-specific intensification of therapy, and then with a discussion on how the impressive efficacy of LCSD should translate into guideline-directed therapy in both current and future guidelines, in order to upgrade the quality of care in the era of precision medicine.
Keywords: Cardiac sympathetic denervation; Catecholaminergic polymorphic ventricular tachycardia; Genetic disorders; Left cardiac sympathetic denervation; Long QT syndrome; Sudden cardiac death.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Lown B. Sudden cardiac death: the major challenge confronting contemporary cardiology. Am J Cardiol 1979;43:313–328. - PubMed
-
- Schwartz PJ. 1970–2020: 50 years of research on the long QT syndrome—from almost zero knowledge to precision medicine. Eur Heart J 2021;42:1063–1072. - PubMed
-
- Collura CA, Johnson JN, Moir C, Ackerman MJ. Left cardiac sympathetic denervation for the treatment of long QT syndrome and catecholaminergic polymorphic ventricular tachycardia using video-assisted thoracic surgery. Heart Rhythm 2009;6:752–759. - PubMed
-
- Schwartz PJ. Cutting nerves and saving lives. Heart Rhythm 2009;6:760–763. - PubMed
