

Mapping ongoing nutrition intervention trials in muscle, sarcopenia, and cachexia: a scoping review of future research
- PMID: 35301816
- PMCID: PMC9178172
- DOI: 10.1002/jcsm.12954
Mapping ongoing nutrition intervention trials in muscle, sarcopenia, and cachexia: a scoping review of future research
Abstract
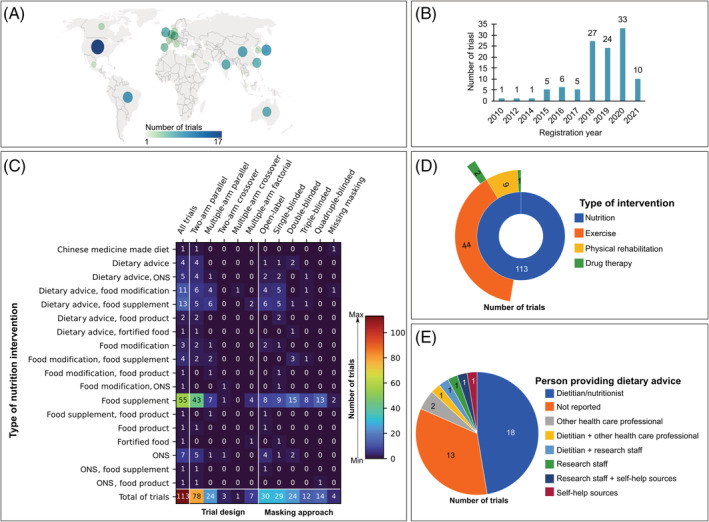
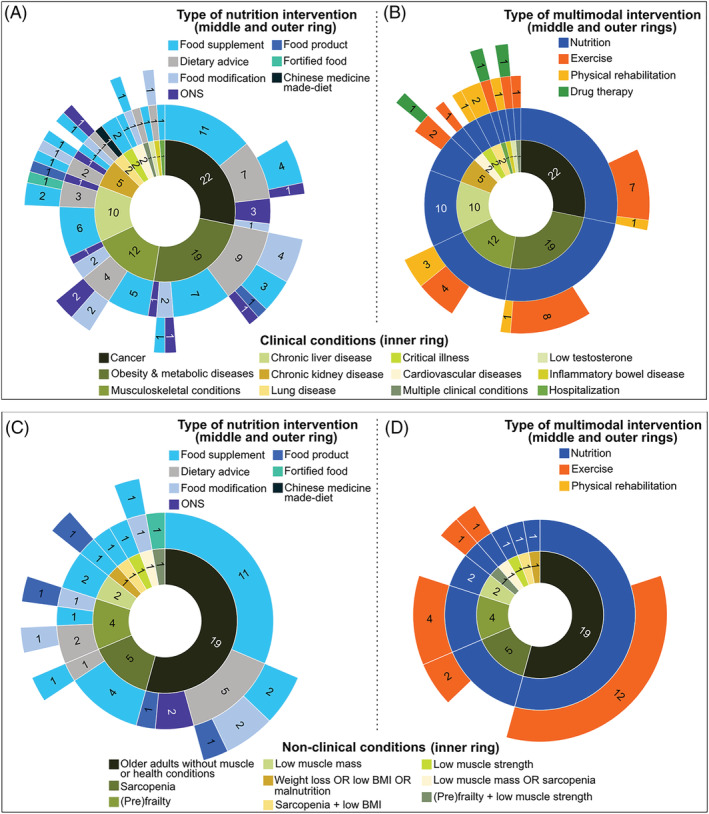
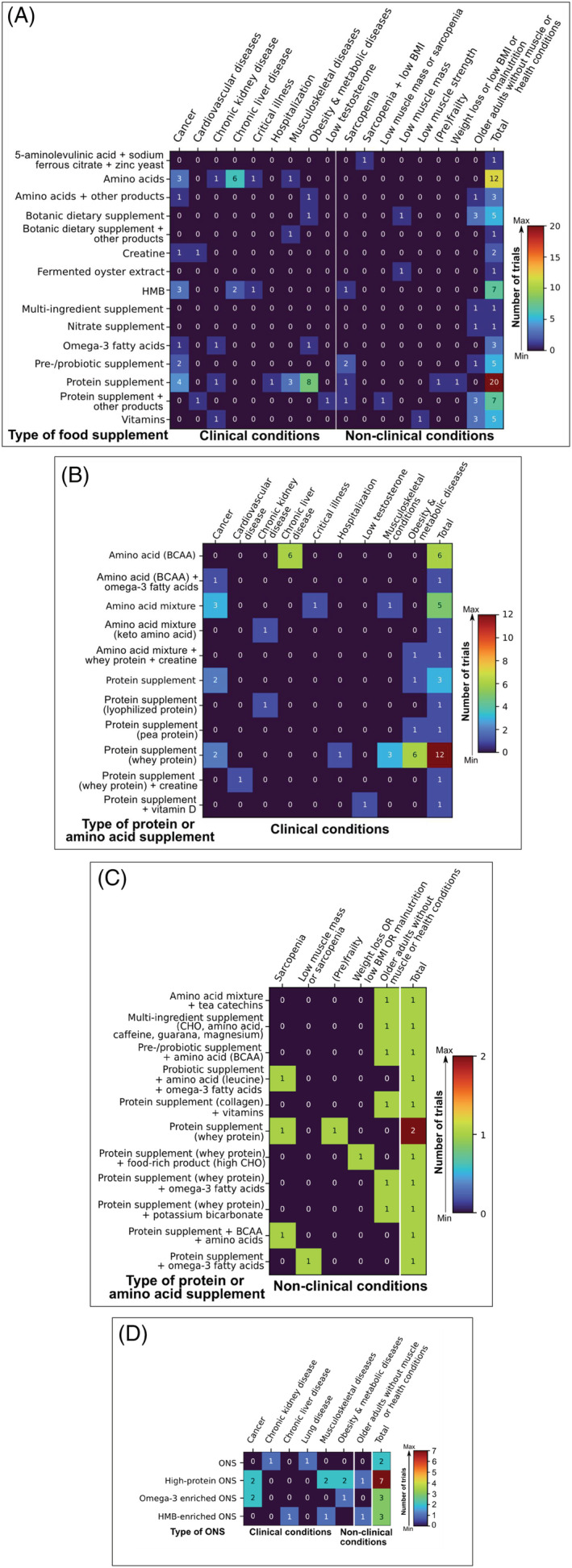
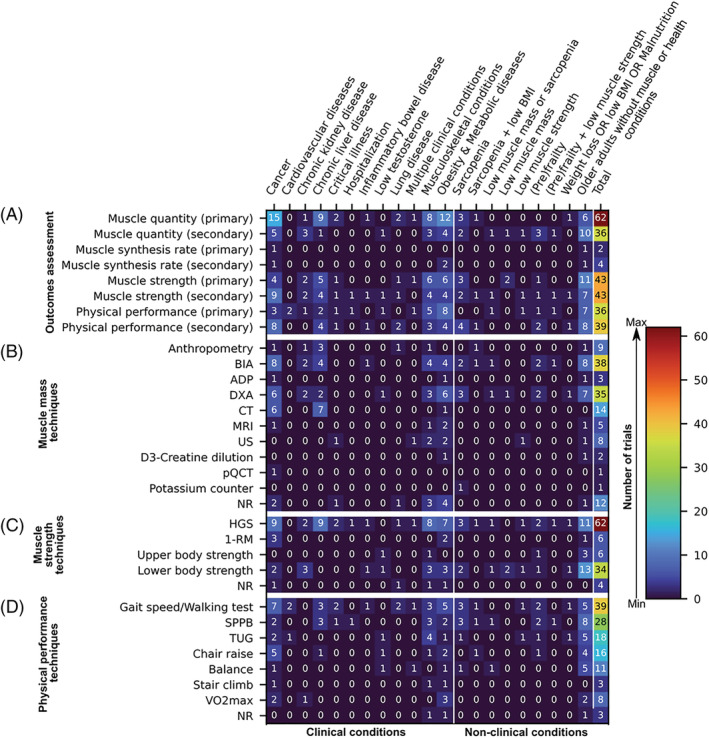
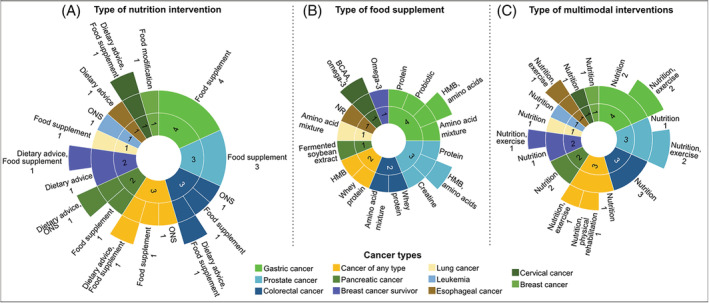
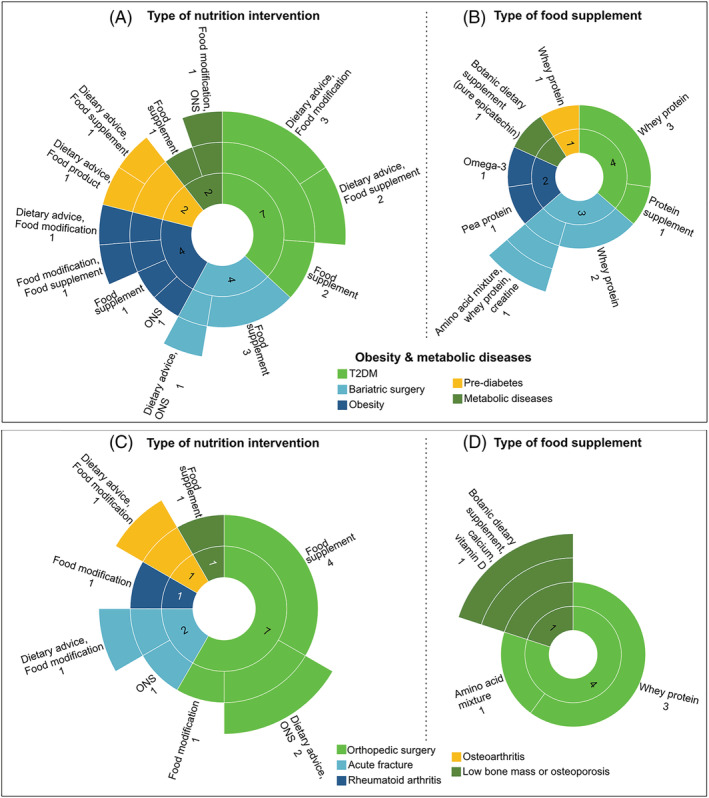
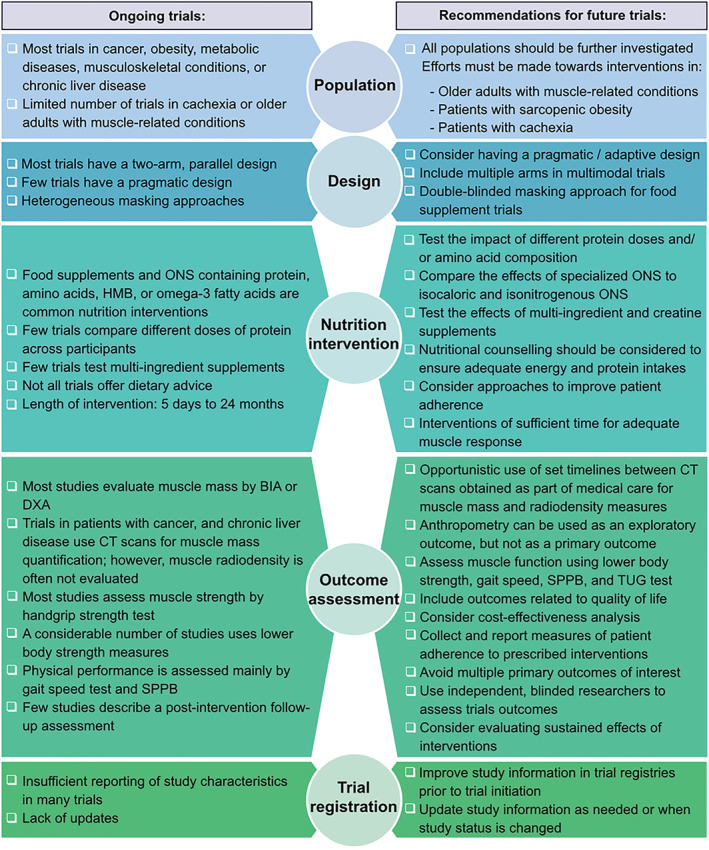
Muscle loss alone, or in the context of sarcopenia or cachexia, is a prevalent condition and a predictor of negative outcomes in aging and disease. As adequate nutrition is essential for muscle maintenance, a growing number of studies has been conducted to explore the role of specific nutrients on muscle mass or function. Nonetheless, more research is needed to guide evidence-based recommendations. This scoping review aimed to compile and document ongoing clinical trials investigating nutrition interventions as a strategy to prevent or treat low muscle mass or function (strength and physical performance), sarcopenia, or cachexia. ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform were searched up to 21 April 2021 for planned and ongoing trials. Randomized controlled trials with ≥20 participants per arm were included based on intent to explore the effects of nutrition interventions on muscle-related outcomes (i.e. muscle mass or strength, physical performance, or muscle synthesis rate) in both clinical and non-clinical conditions (i.e. aging). Two reviewers independently screened records for eligibility, and a descriptive synthesis of trials characteristics was conducted. A total of 113 trials were included in the review. Most trials (69.0%) enroll adults with clinical conditions, such as cancer (19.5%), obesity and metabolic diseases (16.8%), and musculoskeletal diseases (10.7%). The effects of nutrition interventions on age-related muscle loss are explored in 31% of trials. Although nutrition interventions of varied types were identified, food supplements alone (48.7%) or combined with dietary advice (11.5%) are most frequently reported. Protein (17.7%), amino acids (10.6%), and β-hydroxy-β-methylbutyrate (HMB, 6.2%) are the top three food supplements' nutrients under investigation. Primary outcome of most trials (54.9%) consists of measures of muscle mass alone or in combination with muscle strength and/or performance (as either primary or secondary outcomes). Muscle strength and physical performance are primary outcomes of 38% and 31.9% of the trials, respectively. These measurements were obtained using a variety of techniques. Only a few trials evaluate muscle synthesis rate either as a primary or secondary outcome (5.3%). Several nutrition studies focusing on muscle, sarcopenia, and cachexia are underway and can inform future research in this area. Although many trials have similar type of interventions, methodological heterogeneity may challenge study comparisons, and future meta-analyses aiming to provide evidence-based recommendations. Upcoming research in this area may benefit from guidelines for the assessment of therapeutic effects of nutrition interventions.
Keywords: Cachexia; Clinical trials; Dietary intervention; Muscle; Nutrition intervention; Sarcopenia.
© 2022 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
C.E.O. has received honoraria from Abbott Nutrition outside the scope of the submitted work. C.M.P. has received honoraria and/or paid consultancy from Abbott Nutrition, Nutricia, Nestlé Health Science, Fresenius Kabi, Pfizer, and Helsinn. A.L. has received honoraria and/or paid consultancy from Abbott, Baxter, BBraun, Fresenius Kabi, Nestlé Health Science, Nutricia, and Smartfish; and research grant from Fresenius Kabi. The other authors declare that they have no known conflicts of interest.
Figures
References
-
- Mayhew AJ, Amog K, Phillips S, Parise G, McNicholas PD, De Souza RJ, et al. The prevalence of sarcopenia in community‐dwelling older adults, an exploration of differences between studies and within definitions: a systematic review and meta‐analyses. Age Ageing 2019;48:48–56. - PubMed
-
- Ligthart‐Melis GC, Luiking YC, Kakourou A, Cederholm T, Maier AB, de van der Schueren MAE. Frailty, sarcopenia, and malnutrition frequently (Co‐)occur in hospitalized older adults: a systematic review and meta‐analysis. J Am Med Dir Assoc 2020;21:1216–1228. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
