

Impact of Right Ventricular Pressure Load After Repair of Tetralogy of Fallot
- PMID: 35301850
- PMCID: PMC9075442
- DOI: 10.1161/JAHA.121.022694
Impact of Right Ventricular Pressure Load After Repair of Tetralogy of Fallot
Abstract
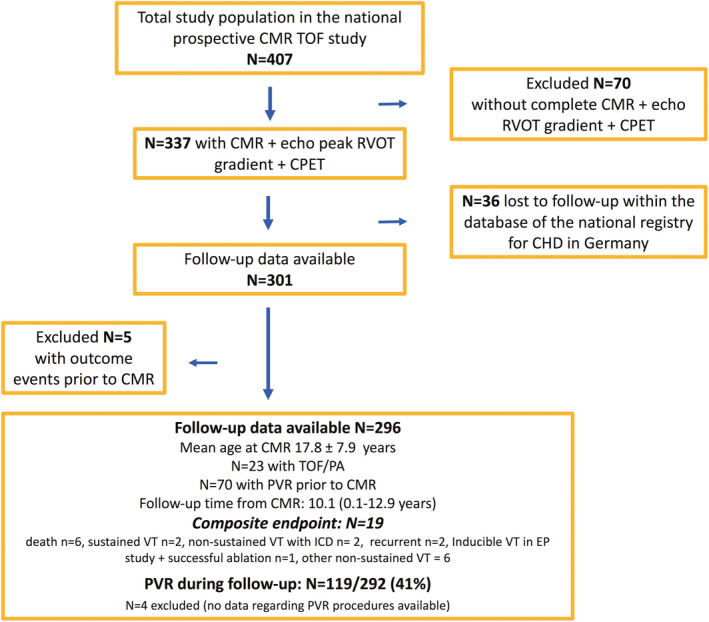
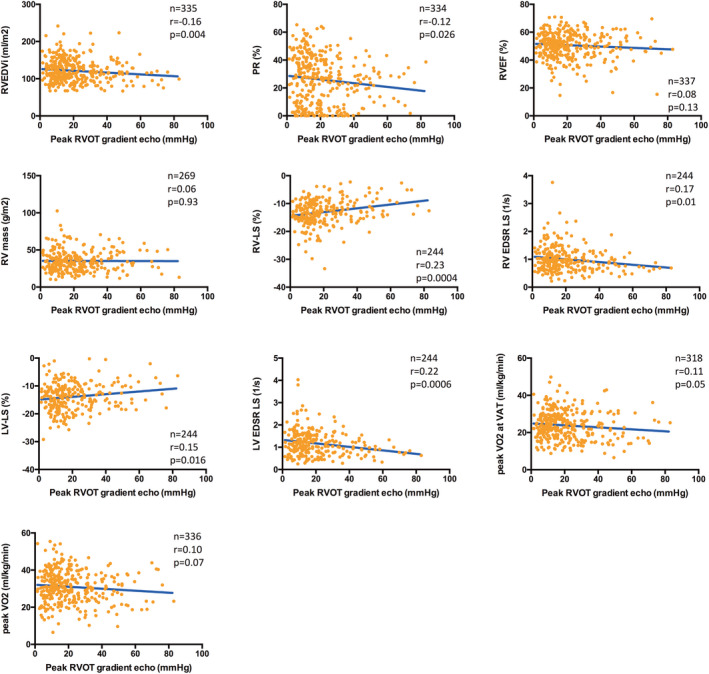
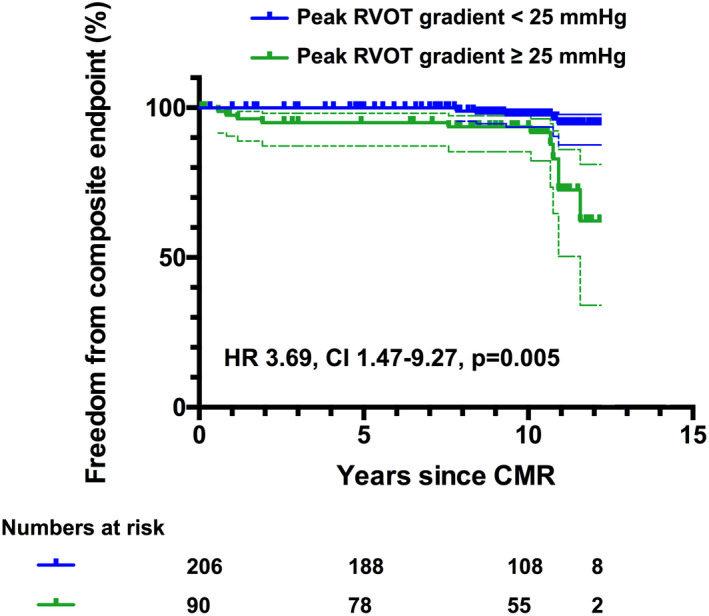
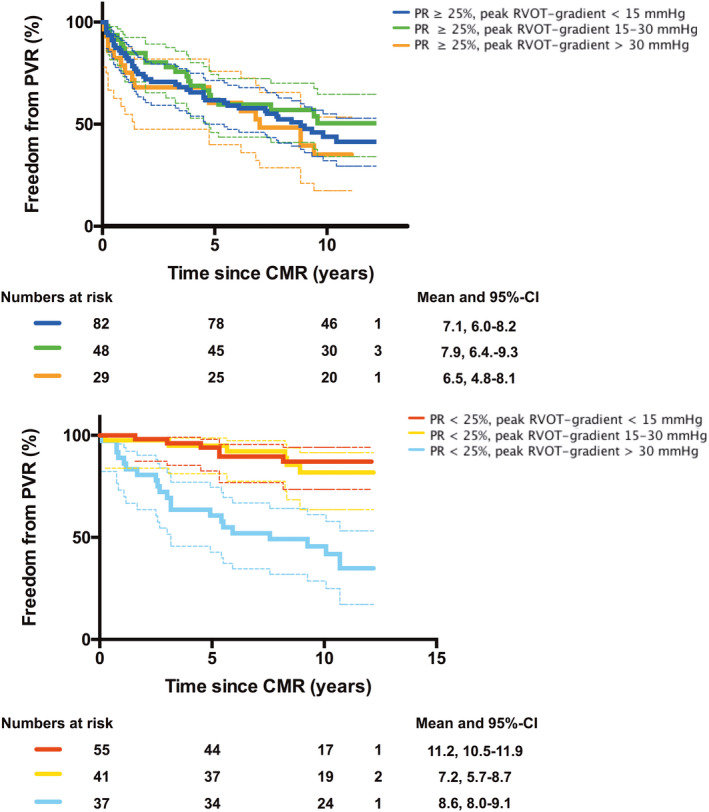
Background Right ventricular outflow tract (RVOT) stenosis after repair of tetralogy of Fallot has been linked with favorable right ventricular remodeling but adverse outcomes. The aim of our study was to assess the hemodynamic impact and prognostic relevance of right ventricular pressure load in this population. Methods and Results A total of 296 patients with repaired tetralogy of Fallot (mean age, 17.8±7.9 years) were included in a prospective cardiovascular magnetic resonance multicenter study. Myocardial strain was quantified by feature tracking technique at study entry. Follow-up, including the need for pulmonary valve replacement, was assessed. The combined end point consisted of ventricular tachycardia and cardiac death. A higher echocardiographic RVOT peak gradient was significantly associated with smaller right ventricular volumes and less pulmonary regurgitation, but lower biventricular longitudinal strain. During a follow-up of 10.1 (0.1-12.9) years, the primary end point was reached in 19 of 296 patients (cardiac death, n=6; sustained ventricular tachycardia, n=2; and nonsustained ventricular tachycardia, n=11). A higher RVOT gradient was associated with the combined outcome (hazard ratio [HR], 1.03; 95% CI, 1.00-1.06; P=0.026), and a cutoff gradient of ≥25 mm Hg was predictive for cardiovascular events (HR, 3.69; 95% CI, 1.47-9.27; P=0.005). In patients with pulmonary regurgitation ≥25%, a mild residual RVOT gradient (15-30 mm Hg) was not associated with a lower risk for pulmonary valve replacement. Conclusions Higher RVOT gradients were associated with less pulmonary regurgitation and smaller right ventricular dimensions but were related to reduced biventricular strain and emerged as univariate predictors of adverse events. Mild residual pressure gradients did not protect from pulmonary valve replacement. These results may have implications for the indication for RVOT reintervention in this population.
Keywords: magnetic resonance imaging; prognosis; right ventricular pressure overload; strain; tetralogy of Fallot.
Figures
References
-
- Davlouros PA, Kilner PJ, Hornung TS, Li W, Francis JM, Moon JC, Smith GC, Tat T, Pennell DJ, Gatzoulis MA. Right ventricular function in adults with repaired tetralogy of Fallot assessed with cardiovascular magnetic resonance imaging: detrimental role of right ventricular outflow aneurysms or akinesia and adverse right‐to‐left ventricular interaction. J Am Coll Cardiol. 2002;40:2044–2052. doi: 10.1016/S0735-1097(02)02566-4 - DOI - PubMed
-
- Boni L, García E, Galletti L, Pérez A, Herrera D, Ramos V, Marianeschi SM, Comas JV. Current strategies in tetralogy of Fallot repair: pulmonary valve sparing and evolution of right ventricle/left ventricle pressures ratio. Eur J Cardio‐Thorac Surg. 2009;35:885–889; discussion 889‐890. doi: 10.1016/j.ejcts.2009.01.016 - DOI - PubMed
-
- Spiewak M, Biernacka EK, Małek LA, Petryka J, Kowalski M, Miłosz B, Zabicka M, Miśko J, Rużyłło W. Right ventricular outflow tract obstruction as a confounding factor in the assessment of the impact of pulmonary regurgitation on the right ventricular size and function in patients after repair of tetralogy of Fallot. J Magn Reson Imaging: JMRI. 2011;33:1040–1046. doi: 10.1002/jmri.22532 - DOI - PubMed
-
- Yoo BW, Kim JO, Kim YJ, Choi JY, Park HK, Park YH, Sul JH. Impact of pressure load caused by right ventricular outflow tract obstruction on right ventricular volume overload in patients with repaired tetralogy of Fallot. J Thorac Cardiovasc Surg. 2012;143:1299–1304. doi: 10.1016/j.jtcvs.2011.12.033 - DOI - PubMed
-
- Latus H, Gummel K, Rupp S, Valeske K, Akintuerk H, Jux C, Bauer J, Schranz D, Apitz C. Beneficial effects of residual right ventricular outflow tract obstruction on right ventricular volume and function in patients after repair of tetralogy of Fallot. Pediatr Cardiol. 2013;34:424–430. doi: 10.1007/s00246-012-0476-4 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
