

Prevalence of Coronary Microvascular Disease and Coronary Vasospasm in Patients With Nonobstructive Coronary Artery Disease: Systematic Review and Meta-Analysis
- PMID: 35301851
- PMCID: PMC9075440
- DOI: 10.1161/JAHA.121.023207
Prevalence of Coronary Microvascular Disease and Coronary Vasospasm in Patients With Nonobstructive Coronary Artery Disease: Systematic Review and Meta-Analysis
Abstract
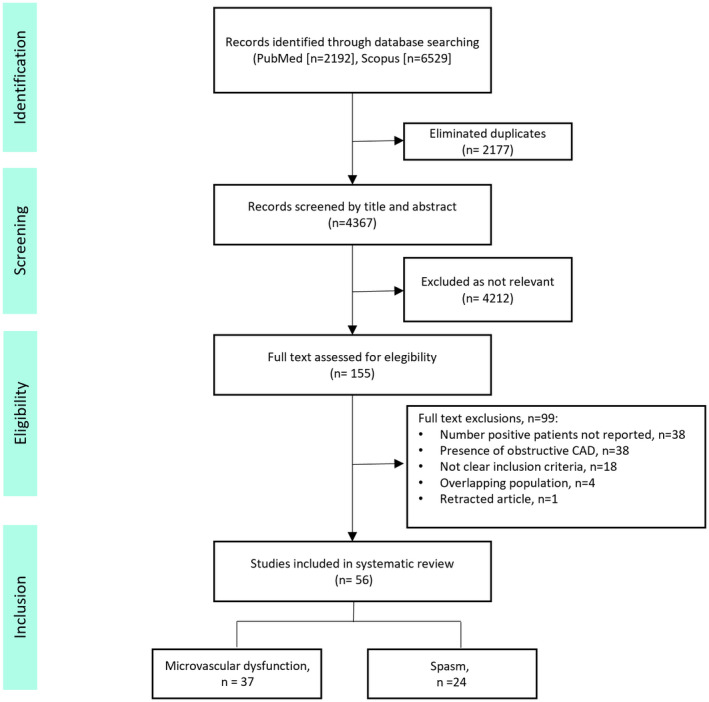
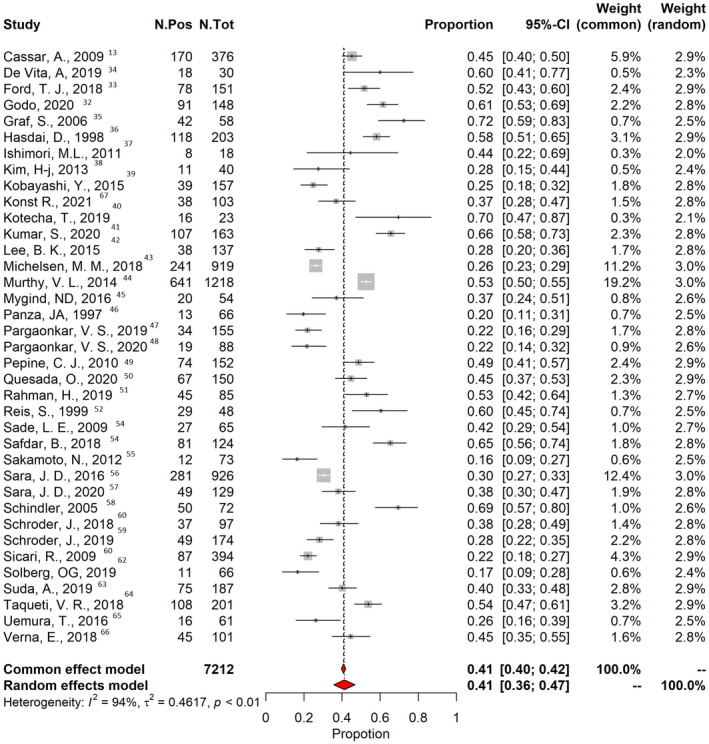
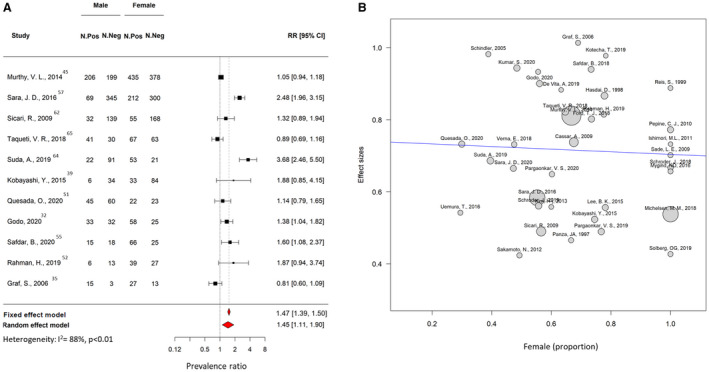
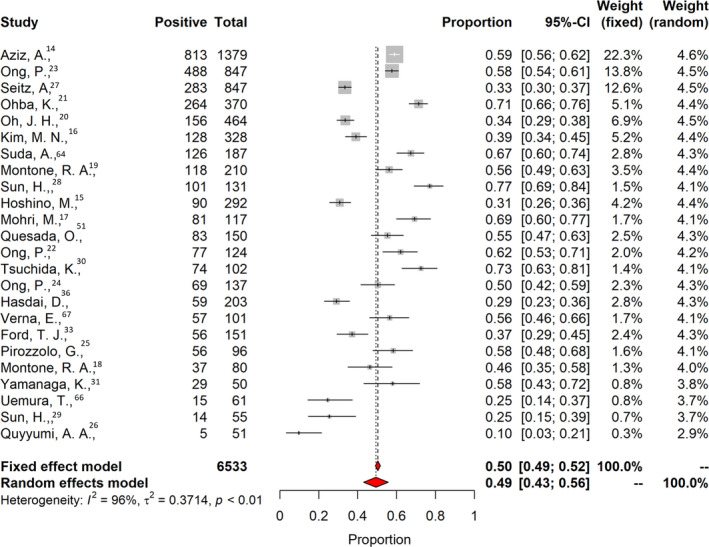
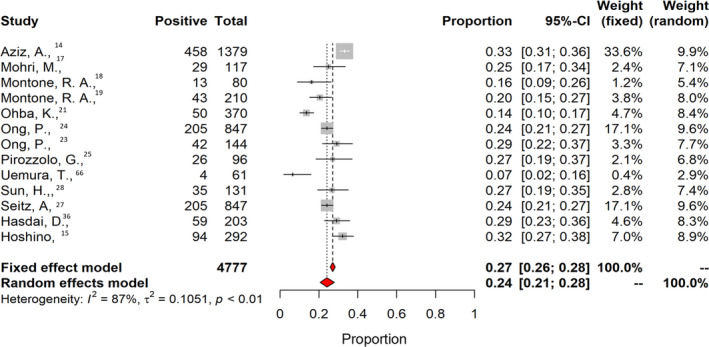
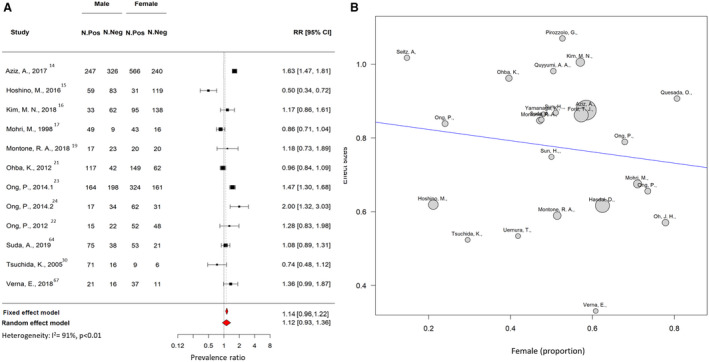
Background A relevant proportion of patients with suspected coronary artery disease undergo invasive coronary angiography showing normal or nonobstructive coronary arteries. However, the prevalence of coronary microvascular disease (CMD) and coronary spasm in patients with nonobstructive coronary artery disease remains to be determined. The objective of this study was to determine the prevalence of coronary CMD and coronary vasospastic angina in patients with no obstructive coronary artery disease. Methods and Results A systematic review and meta-analysis of studies assessing the prevalence of CMD and vasospastic angina in patients with no obstructive coronary artery disease was performed. Random-effects models were used to determine the prevalence of these 2 disease entities. Fifty-six studies comprising 14 427 patients were included. The pooled prevalence of CMD was 0.41 (95% CI, 0.36-0.47), epicardial vasospasm 0.40 (95% CI, 0.34-0.46) and microvascular spasm 24% (95% CI, 0.21-0.28). The prevalence of combined CMD and vasospastic angina was 0.23 (95% CI, 0.17-0.31). Female patients had a higher risk of presenting with CMD compared with male patients (risk ratio, 1.45 [95% CI, 1.11-1.90]). CMD prevalence was similar when assessed using noninvasive or invasive diagnostic methods. Conclusions In patients with no obstructive coronary artery disease, approximately half of the cases were reported to have CMD and/or coronary spasm. CMD was more prevalent among female patients. Greater awareness among physicians of ischemia with no obstructive coronary arteries is urgently needed for accurate diagnosis and patient-tailored management.
Keywords: angina with nonobstructive coronary artery disease; ischemia with no obstructive coronary artery disease; vasospastic angina.
Figures

References
-
- Khan MAB, Hashim MJ, Mustafa H, Baniyas MY, Al Suwaidi SKBM, AlKatheeri R, Alblooshi FMK, Almatrooshi MEAH, Alzaabi MEH, Al Darmaki RS, et al. Global epidemiology of ischemic heart disease: results from the Global Burden of Disease Study. Cureus. 2020;12:e9349. doi: 10.7759/cureus.9349 - DOI - PMC - PubMed
-
- Jespersen L, Hvelplund A, Abildstrøm SZ, Pedersen F, Galatius S, Madsen JK, Jørgensen E, Kelbæk H, Prescott E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734–744. doi: 10.1093/eurheartj/ehr331 - DOI - PubMed
-
- Da Costa A, Isaaz K, Faure E, Mourot S, Cerisier A, Lamaud M. Clinical characteristics, aetiological factors and long‐term prognosis of myocardial infarction with an absolutely normal coronary angiogram; a 3‐year follow‐up study of 91 patients. Eur Heart J. 2001;22:1459–1465. doi: 10.1053/euhj.2000.2553 - DOI - PubMed
-
- Radico F, Zimarino M, Fulgenzi F, Ricci F, Di Nicola M, Jespersen L, Chang SM, Humphries KH, Marzilli M, De Caterina R. Determinants of long‐term clinical outcomes in patients with angina but without obstructive coronary artery disease: a systematic review and meta‐analysis. Eur Heart J. 2018;39:2135–2146. doi: 10.1093/eurheartj/ehy185 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
