

Preintubation Sequential Organ Failure Assessment Score for Predicting COVID-19 Mortality: External Validation Using Electronic Health Record From 86 U.S. Healthcare Systems to Appraise Current Ventilator Triage Algorithms
- PMID: 35302957
- PMCID: PMC9196924
- DOI: 10.1097/CCM.0000000000005534
Preintubation Sequential Organ Failure Assessment Score for Predicting COVID-19 Mortality: External Validation Using Electronic Health Record From 86 U.S. Healthcare Systems to Appraise Current Ventilator Triage Algorithms
Abstract
Objectives: Prior research has hypothesized the Sequential Organ Failure Assessment (SOFA) score to be a poor predictor of mortality in mechanically ventilated patients with COVID-19. Yet, several U.S. states have proposed SOFA-based algorithms for ventilator triage during crisis standards of care. Using a large cohort of mechanically ventilated patients with COVID-19, we externally validated the predictive capacity of the preintubation SOFA score for mortality prediction with and without other commonly used algorithm elements.
Design: Multicenter, retrospective cohort study using electronic health record data.
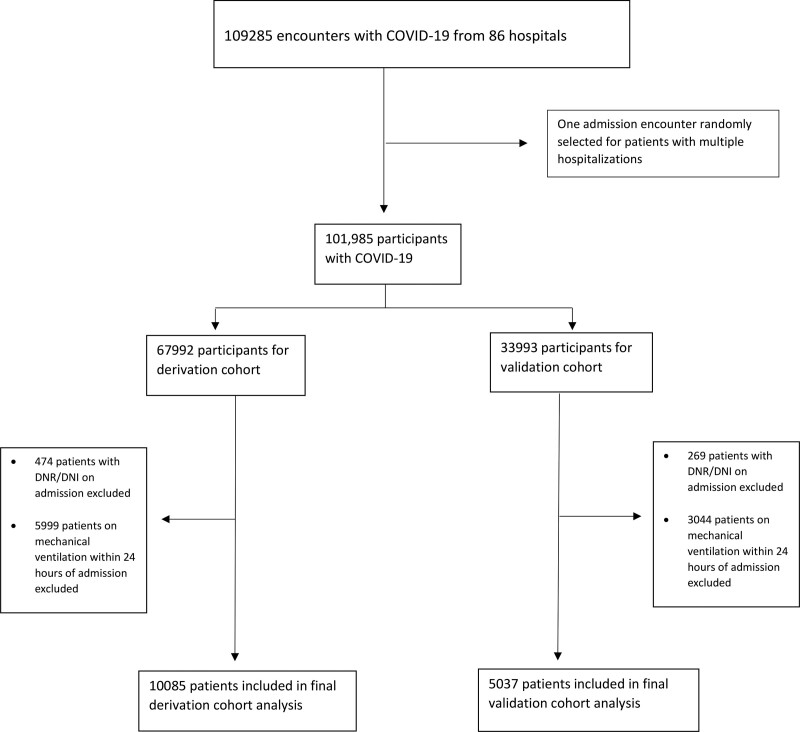
Setting: Eighty-six U.S. health systems.
Patients: Patients with COVID-19 hospitalized between January 1, 2020, and February 14, 2021, and subsequently initiated on mechanical ventilation.
Interventions: None.
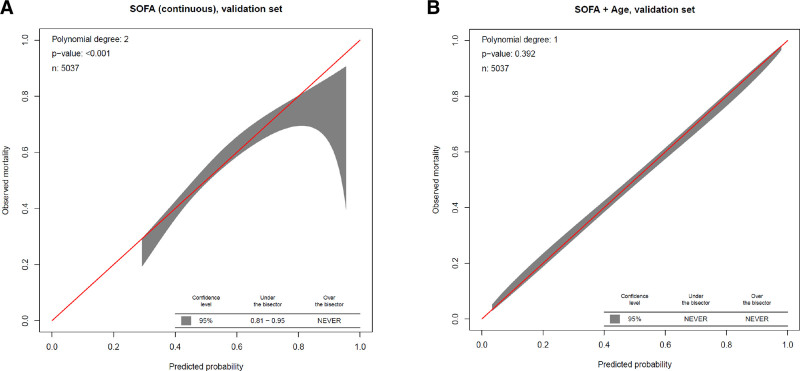
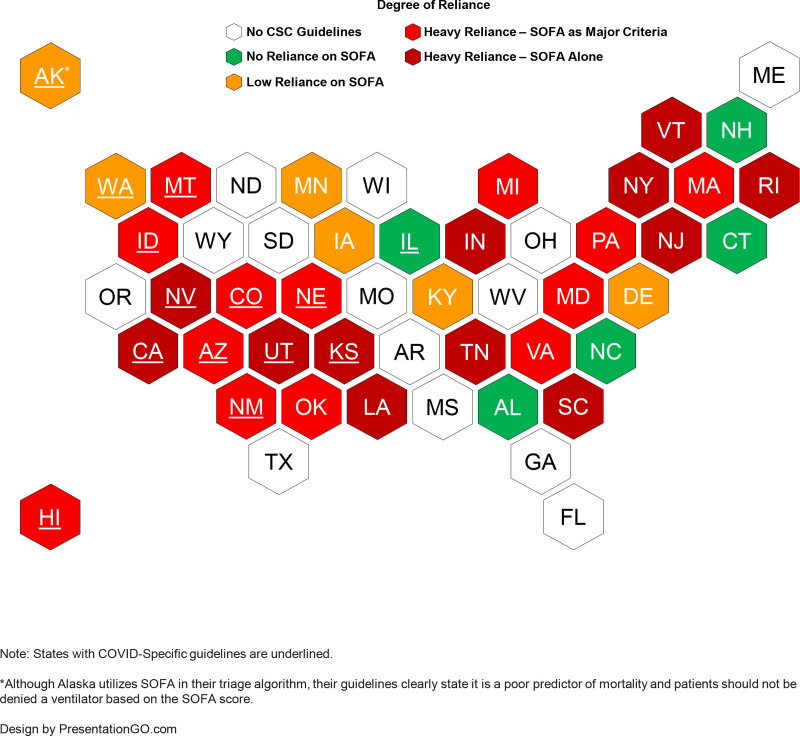
Measurements and main results: Among 15,122 mechanically ventilated patients with COVID-19, SOFA score alone demonstrated poor discriminant accuracy for inhospital mortality in mechanically ventilated patients using the validation cohort (area under the receiver operating characteristic curve [AUC], 0.66; 95% CI, 0.65-0.67). Discriminant accuracy was even poorer using SOFA score categories (AUC, 0.54; 95% CI, 0.54-0.55). Age alone demonstrated greater discriminant accuracy for inhospital mortality than SOFA score (AUC, 0.71; 95% CI, 0.69-0.72). Discriminant accuracy for mortality improved upon addition of age to the continuous SOFA score (AUC, 0.74; 95% CI, 0.73-0.76) and categorized SOFA score (AUC, 0.72; 95% CI, 0.71-0.73) models, respectively. The addition of comorbidities did not substantially increase model discrimination. Of 36 U.S. states with crisis standards of care guidelines containing ventilator triage algorithms, 31 (86%) feature the SOFA score. Of these, 25 (81%) rely heavily on the SOFA score (12 exclusively propose SOFA; 13 place highest weight on SOFA or propose SOFA with one other variable).
Conclusions: In a U.S. cohort of over 15,000 ventilated patients with COVID-19, the SOFA score displayed poor predictive accuracy for short-term mortality. Our findings warrant reappraisal of the SOFA score's implementation and weightage in existing ventilator triage pathways in current U.S. crisis standards of care guidelines.
Copyright © 2022 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Figures
Comment in
-
Predictive Algorithms for a Crisis.Crit Care Med. 2022 Jul 1;50(7):1150-1153. doi: 10.1097/CCM.0000000000005550. Epub 2022 Jun 13. Crit Care Med. 2022. PMID: 35726979 Free PMC article. No abstract available.
References
-
- Committee on Guidance for Establishing Crisis Standards of Care for Use in Disaster S, Institute of M: In: Crisis Standards of Care: A Systems Framework for Catastrophic Disaster Response. Washington, DC, National Academies Press, 2012 - PubMed
-
- New York State Task Force on Life and the Law New York State Department of Health: Ventilator allocation guidelines. 2015. Available at: https://www.health.ny.gov/regulations/task_force/reports_publications/do.... Accessed October 1, 2021
-
- Washington State Department of Health, Northwest Healthcare Response Network: Scarce resource management & crisis standards of care. 2020. Available at: https://nwhrn.org/wp-content/uploads/2020/03/Scarce_Resource_Management_.... Accessed October 1, 2021
-
- University of Pittsburgh: Allocation of scarce critical care resources during a public health emergency. 2020. Available at: https://ccm.pitt.edu/sites/default/files/UnivPittsburgh_ModelHospitalRes.... Accessed October 1, 2021
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
