

Conspicuity and muscle-invasiveness assessment for bladder cancer using VI-RADS: a multi-reader, contrast-free MRI study to determine optimal b-values for diffusion-weighted imaging
- PMID: 35303112
- PMCID: PMC9038787
- DOI: 10.1007/s00261-022-03490-9
Conspicuity and muscle-invasiveness assessment for bladder cancer using VI-RADS: a multi-reader, contrast-free MRI study to determine optimal b-values for diffusion-weighted imaging
Abstract
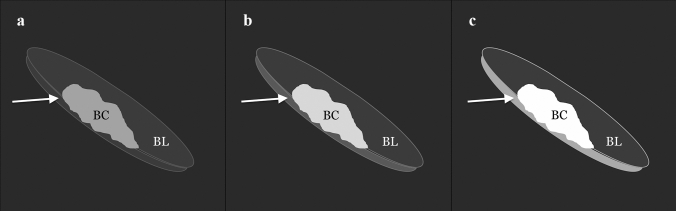
Objective: To (1) compare bladder cancer (BC) muscle invasiveness among three b-values using a contrast-free approach based on Vesical Imaging-Reporting and Data System (VI-RADS), to (2) determine if muscle-invasiveness assessment is affected by the reader experience, and to (3) compare BC conspicuity among three b-values, qualitatively and quantitatively.
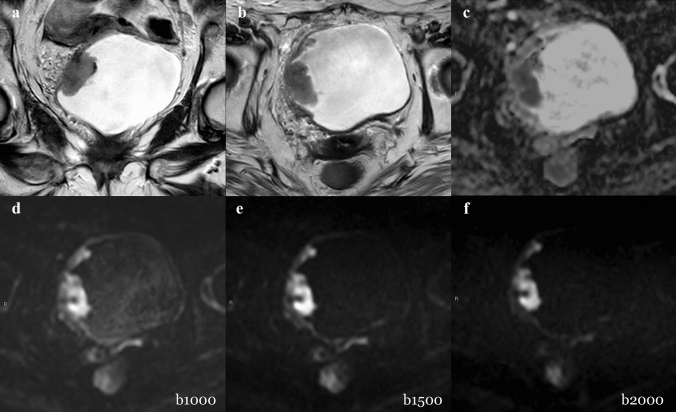
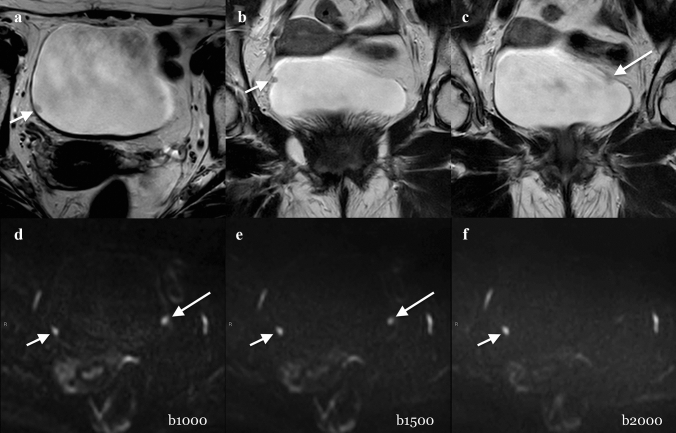
Methods: Thirty-eight patients who underwent a bladder MRI on a 3.0-T scanner were enrolled. The gold standard was histopathology report following transurethral resection of BC. Three sets of images, including T2w and different b-values for DWI, set 1 (b = 1000 s/mm2), set 2 (b = 1500 s/mm2), and set 3 (b = 2000 s/mm2), were reviewed by three differently experienced readers. Descriptive statistics and Intraclass Correlation Coefficient (ICC) were calculated. Comparisons among readers and DWI sets were performed with the Wilcoxon test. Receiver operating characteristic (ROC) analysis was performed. Areas under the curves (AUCs) and pairwise comparison were calculated.
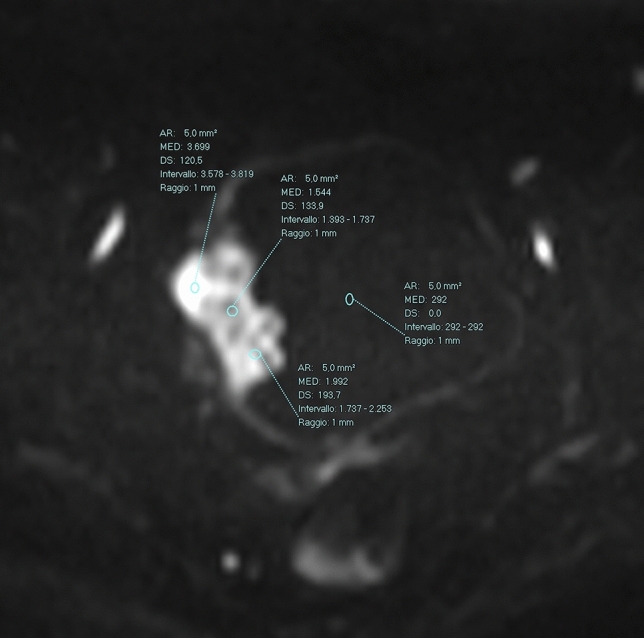
Results: AUCs of muscle-invasiveness assessment ranged from 0.896 to 0.984 (reader 1), 0.952-0.968 (reader 2), and 0.952-0.984 (reader 3) without significant differences among different sets and readers (p > 0.05). The mean conspicuity qualitative scores were higher in Set 1 (2.21-2.33), followed by Set 2 (2-2.16) and Set 3 (1.82-2.14). The quantitative conspicuity assessment showed that mean normalized intensity of tumor was significantly higher in Set 2 (4.217-4.737) than in Set 1 (3.923-4.492) and Set 3 (3.833-3.992) (p < 0.05).
Conclusion: Muscle invasiveness can be assessed with high accuracy using a contrast-free protocol with T2W and DWI, regardless of reader's experience. b = 1500 s/mm2 showed the best tumor delineation, while b = 1000 s/mm2 allowed for better tumor-wall interface assessment.
Keywords: Bladder cancer; Diffusion-weighted imaging; MRI; VI-RADS.
© 2022. The Author(s).
Conflict of interest statement
Domenico Mastrodicasa had no activities related to the present article. Activities not related to the present article: shareholder of Segmed, Inc. and consultant for Segmed, Inc. All the other authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. Andrea Delli Pizzi is a member of the Scientific Editorial Board of Insight Into Imaging.
Figures
References
-
- Palumbo C, Mistretta FA, Knipper S, Pecoraro A, Tian Z, Shariat SF, et al. How cancer-specific mortality changes over time after radical cystectomy: Conditional survival of patients with nonmetastatic urothelial carcinoma of the urinary bladder. Urol Oncol. 2019;37:893–899. doi: 10.1016/j.urolonc.2019.05.020. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
