

Community-based rehabilitation intervention for people with schizophrenia in Ethiopia (RISE): results of a 12-month cluster-randomised controlled trial
- PMID: 35303462
- PMCID: PMC8938762
- DOI: 10.1016/S2214-109X(22)00027-4
Community-based rehabilitation intervention for people with schizophrenia in Ethiopia (RISE): results of a 12-month cluster-randomised controlled trial
Erratum in
-
Correction to Lancet Glob Health 2022; 10: e530-42.Lancet Glob Health. 2022 Jun;10(6):e797. doi: 10.1016/S2214-109X(22)00216-9. Lancet Glob Health. 2022. PMID: 35561718 Free PMC article. No abstract available.
Abstract
Background: Community-based rehabilitation (CBR) is recommended to address the social and clinical needs of people with schizophrenia in resource-poor settings. We evaluated the effectiveness of CBR at reducing disability at 12 months in people with schizophrenia who had disabling illness after having had the opportunity to access facility-based care for 6 months METHODS: This cluster-randomised controlled trial was conducted in a rural district of Ethiopia. Eligible clusters were subdistricts in Sodo district that had not participated in the pilot study. Available subdistricts were randomised (in a 1:1 ratio) to either the intervention group (CBR plus facility-based care) or to the control group (facility-based care alone). An optimisation procedure (accounting for the subdistrict mean WHO Disability Assessment Schedule (WHODAS) score and the potential number of participants per subdistrict) was applied for each of the eight health facilities in the district. An independent statistician, masked to the intervention or control label, used a computer programme to randomly choose the allocation sequence from the set of optimal ones. We recruited adults with disabling illness as a result of schizophrenia. The subdistricts were eligible for inclusion if they included participants that met the eligibility criteria. Researchers recruiting and assessing participants were masked to allocation status. Facility-based care was a task-shared model of mental health care integrated within primary care. CBR was delivered by lay workers over a 12-month period, comprising of home visits (psychoeducation, adherence support, family intervention, and crisis management) and community mobilisation. The primary outcome was disability, measured with the proxy-rated 36-item WHODAS score at 12 months. The subdistricts that had primary outcome data available were included in the primary analysis. This study is registered with ClinicalTrials.gov, NCT02160249.
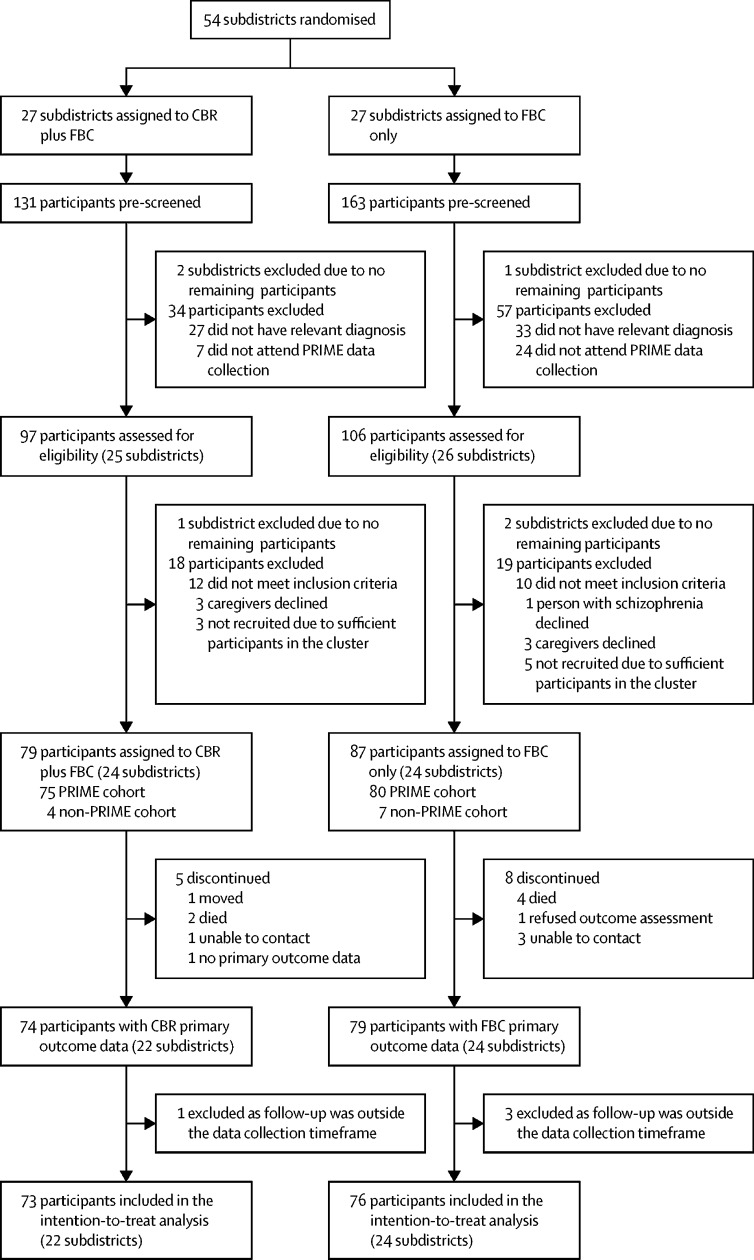
Findings: Enrolment took place between Sept 16, 2015 and Mar 11, 2016. 54 subdistricts were randomised (27 to the CBR plus facility-based care group and 27 to the facility-based care group). After exclusion of subdistricts without eligible participants, we enrolled 79 participants (66% men and 34% women) from 24 subdistricts assigned to CBR plus facility-based care and 87 participants (59% men and 41% women) from 24 subdistricts assigned to facility-based care only. The primary analysis included 149 (90%) participants in 46 subdistricts (73 participants in 22 subdistricts in the CBR plus facility-based care group and 76 participants in 24 subdistricts in the facility-based care group). At 12 months, the mean WHODAS scores were 46·1 (SD 23·3) in the facility-based care group and 40·6 (22·5) in the CBR plus facility-based care group, indicating a favourable intervention effect (adjusted mean difference -8·13 [95% CI -15·85 to -0·40]; p=0·039; effect size 0·35). Four (5%) CBR plus facility-based care group participants and nine (10%) facility-based care group participants had one or more serious adverse events (death, suicide attempt, and hospitalisation).
Interpretation: CBR delivered by lay workers combined with task-shared facility-based care, was effective in reducing disability among people with schizophrenia. The RISE study CBR model is particularly relevant to low-income countries with few mental health specialists.
Funding: Wellcome Trust.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests CH reports support from the National Institute of Health Research (NIHR) through a RIGHT grant (NIHR200842) and the NIHR Global Health Research Unit on Health System Strengthening in sub-Saharan Africa, King's College London (GHRU 16/136/54), using aid from the UK Government; and support from African Mental Health Research Initiative as part of the Developing Excellence in Leadership, Training, and Science Africa Initiative (DEL-15–01). HAW reports support from the UK Medical Research Council (MRC) and the UK Department for International Development (DFID) under the MRC-DFID concordat agreement, which is also part of the European and Developing Countries Clinical Trials Partnership programme 2 supported by the EU (MR/R010161/1). All other authors declare no competing interests. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Figures
Comment in
-
Addressing the complex needs of people with severe mental health disorders in low-resource settings.Lancet Glob Health. 2022 Apr;10(4):e457-e458. doi: 10.1016/S2214-109X(22)00092-4. Lancet Glob Health. 2022. PMID: 35303444 No abstract available.
References
-
- WHO . World Health Organization; Geneva: 2010. Community based rehabilitation: CBR guidelines.https://www.who.int/publications/i/item/9789241548052 - PubMed
-
- WHO . World Health Organization; Geneva: 2016. mhGAP Intervention Guide for mental, neurological and substance use disorders in non-specialized health settings Version 2.0.https://www.who.int/publications/i/item/9789241549790 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
