

Acute kidney injury in hospitalized children with sickle cell anemia
- PMID: 35303803
- PMCID: PMC8933904
- DOI: 10.1186/s12882-022-02731-9
Acute kidney injury in hospitalized children with sickle cell anemia
Abstract
Background: Children with sickle cell anemia (SCA) are at increased risk of acute kidney injury (AKI) that may lead to death or chronic kidney disease. This study evaluated AKI prevalence and risk factors in children with SCA hospitalized with a vaso-occlusive crisis (VOC) in a low-resource setting. Further, we evaluated whether modifications to the Kidney Disease: Improving Global Outcomes (KDIGO) definition would influence clinical outcomes of AKI in children with SCA hospitalized with a VOC.
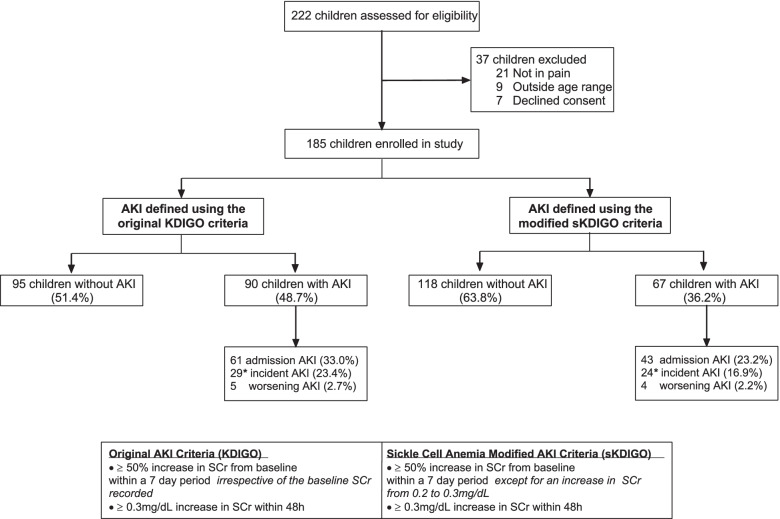
Methods: We prospectively enrolled 185 children from 2 - 18 years of age with SCA (Hemoglobin SS) hospitalized with a VOC at a tertiary hospital in Uganda. Kidney function was assessed on admission, 24-48 h of hospitalization, and day 7 or discharge. Creatinine was measured enzymatically using an isotype-dilution mass spectrometry traceable method. AKI was defined using the original-KDIGO definition as ≥ 1.5-fold change in creatinine within seven days or an absolute change of ≥ 0.3 mg/dl within 48 h. The SCA modified-KDIGO (sKDIGO) definition excluded children with a 1.5-fold change in creatinine from 0.2 mg/dL to 0.3 mg/dL.
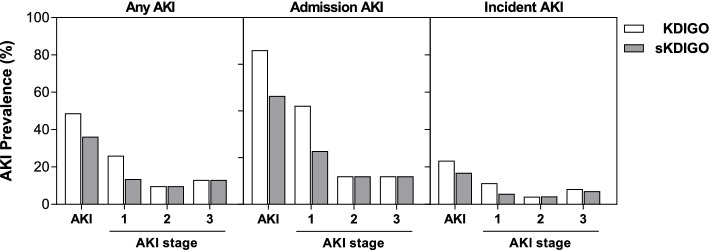
Results: Using KDIGO, 90/185 (48.7%) children had AKI with 61/185 (33.0%) AKI cases present on admission, and 29/124 (23.4%) cases of incident AKI. Overall, 23 children with AKI had a 1.5-fold increase in creatinine from 0.2 mg/dL to 0.3 m/dL. Using the sKDIGO-definition, 67/185 (36.2%) children had AKI with 43/185 (23.2%) cases on admission, and 24/142 (16.9%) cases of incident AKI. The sKDIGO definition, but not the original-KDIGO definition, was associated with increased mortality (0.9% vs. 7.5%, p = 0.024). Using logistic regression, AKI risk factors included age (aOR, 1.10, 95% CI 1.10, 1.20), hypovolemia (aOR, 2.98, 95% CI 1.08, 8.23), tender hepatomegaly (aOR, 2.46, 95% CI 1.05, 5.81), and infection (aOR, 2.63, 95% CI 1.19, 5.81) (p < 0.05).
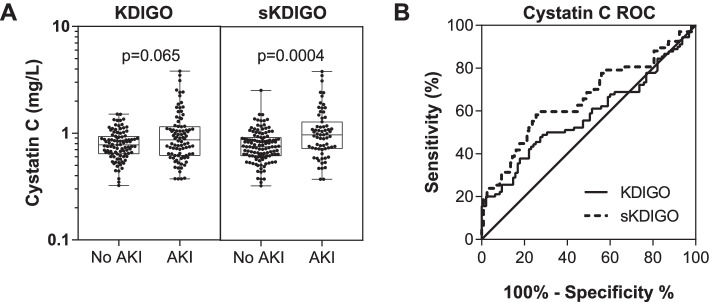
Conclusion: These results demonstrate that AKI is a common complication in children with SCA admitted with VOC. The sKDIGO definition of AKI in children with SCA was a better predictor of clinical outcomes in children. There is need for promotion of targeted interventions to ensure early identification and treatment of AKI in children with SCA.
Keywords: Acute kidney injury; Children; Cystatin C; Hemoglobinuria; Infection; Malaria; Serum creatinine; Sickle cell anemia; Sub-Saharan Africa; Vaso-occlusive crises.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- McCormick M, Richardson T, Warady BA, Novelli EM, Kalpatthi R. Acute kidney injury in paediatric patients with sickle cell disease is associated with increased morbidity and resource utilization. Br J Haematol. 2020;189(3):559–565. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
