

A machine learning-based risk stratification tool for in-hospital mortality of intensive care unit patients with heart failure
- PMID: 35303896
- PMCID: PMC8932070
- DOI: 10.1186/s12967-022-03340-8
A machine learning-based risk stratification tool for in-hospital mortality of intensive care unit patients with heart failure
Abstract
Background: Predicting hospital mortality risk is essential for the care of heart failure patients, especially for those in intensive care units.
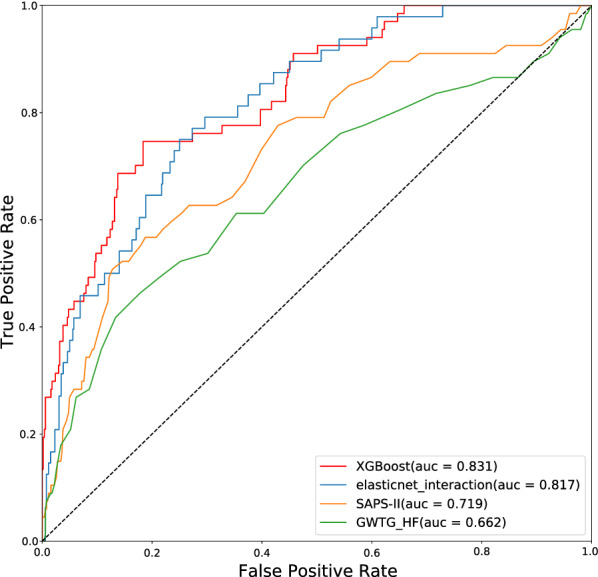
Methods: Using a novel machine learning algorithm, we constructed a risk stratification tool that correlated patients' clinical features and in-hospital mortality. We used the extreme gradient boosting algorithm to generate a model predicting the mortality risk of heart failure patients in the intensive care unit in the derivation dataset of 5676 patients from the Medical Information Mart for Intensive Care III database. The logistic regression model and a common risk score for mortality were used for comparison. The eICU Collaborative Research Database dataset was used for external validation.
Results: The performance of the machine learning model was superior to that of conventional risk predictive methods, with the area under curve 0.831 (95% CI 0.820-0.843) and acceptable calibration. In external validation, the model had an area under the curve of 0.809 (95% CI 0.805-0.814). Risk stratification through the model was specific when the hospital mortality was very low, low, moderate, high, and very high (2.0%, 10.2%, 11.5%, 21.2% and 56.2%, respectively). The decision curve analysis verified that the machine learning model is the best clinically valuable in predicting mortality risk.
Conclusion: Using readily available clinical data in the intensive care unit, we built a machine learning-based mortality risk tool with prediction accuracy superior to that of linear regression model and common risk scores. The risk tool may support clinicians in assessing individual patients and making individualized treatment.
Keywords: Extreme gradient boosting; Heart failure; Machine learning models; Medical information mart for intensive care; Risk stratification.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that have no competing interests.
Figures



Similar articles
-
Prediction model of in-hospital mortality in intensive care unit patients with heart failure: machine learning-based, retrospective analysis of the MIMIC-III database.BMJ Open. 2021 Jul 23;11(7):e044779. doi: 10.1136/bmjopen-2020-044779. BMJ Open. 2021. PMID: 34301649 Free PMC article.
-
A Novel Composite Indicator of Predicting Mortality Risk for Heart Failure Patients With Diabetes Admitted to Intensive Care Unit Based on Machine Learning.Front Endocrinol (Lausanne). 2022 Jun 29;13:917838. doi: 10.3389/fendo.2022.917838. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35846312 Free PMC article.
-
Machine learning-based in-hospital mortality risk prediction tool for intensive care unit patients with heart failure.Front Cardiovasc Med. 2023 Apr 3;10:1119699. doi: 10.3389/fcvm.2023.1119699. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37077747 Free PMC article.
-
Methodological Review of Classification Trees for Risk Stratification: An Application Example in the Obesity Paradox.Nutrients. 2025 May 31;17(11):1903. doi: 10.3390/nu17111903. Nutrients. 2025. PMID: 40507172 Free PMC article. Review.
-
Machine learning in predicting heart failure survival: a review of current models and future prospects.Heart Fail Rev. 2025 Mar;30(2):431-442. doi: 10.1007/s10741-024-10474-y. Epub 2024 Dec 10. Heart Fail Rev. 2025. PMID: 39656330 Review.
Cited by
-
Development and validation of novel interpretable survival prediction models based on drug exposures for severe heart failure during vulnerable period.J Transl Med. 2024 Aug 6;22(1):743. doi: 10.1186/s12967-024-05544-6. J Transl Med. 2024. PMID: 39107765 Free PMC article.
-
Computational approaches in rheumatic diseases - Deciphering complex spatio-temporal cell interactions.Comput Struct Biotechnol J. 2023 Aug 6;21:4009-4020. doi: 10.1016/j.csbj.2023.08.005. eCollection 2023. Comput Struct Biotechnol J. 2023. PMID: 37649712 Free PMC article. Review.
-
Development and validation of a nomogram prediction model for factors influencing 131I-refractory Graves' hyperthyroidism.Front Endocrinol (Lausanne). 2025 Aug 13;16:1628226. doi: 10.3389/fendo.2025.1628226. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40881120 Free PMC article.
-
A machine learning-based severity stratification tool for high altitude pulmonary edema.BMC Med Inform Decis Mak. 2025 Apr 18;25(1):171. doi: 10.1186/s12911-025-02992-y. BMC Med Inform Decis Mak. 2025. PMID: 40251543 Free PMC article.
-
Comparison of the prognostic value, feasibility, and reproducibility among different scoring methods of 8‑point lung ultrasonography in patients with acute heart failure.Intern Emerg Med. 2023 Nov;18(8):2321-2332. doi: 10.1007/s11739-023-03433-2. Epub 2023 Sep 25. Intern Emerg Med. 2023. PMID: 37747589
References
-
- Seferović PM. ESC/HFA guidelines for the diagnosis and treatment of acute and chronic heart failure 2016. J Card Fail. 2017 doi: 10.1016/j.cardfail.2017.08.005. - DOI
-
- Amina G, Amer I, Admir R, Ira T, Selma J, Anes A, Adis K. Predictive value of SAPS II and APACHE II scoring systems for patient outcome in a medical intensive care unit. Acta Med Acad. 2016;45(2):97–103. - PubMed
-
- Izabela K, Rafał Ś, Karolina B, Paweł T, Wojciech S. Validation of APACHE II and SAPS II scales at the intensive care unit along with assessment of SOFA scale at the admission as an isolated risk of death predictor. Anaesthesiol Intensive Therapy. 2019;51(2):107–11. doi: 10.5114/ait.2019.86275. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
