

Management of anterior thigh injuries in soccer players: practical guide
- PMID: 35303927
- PMCID: PMC8932115
- DOI: 10.1186/s13102-022-00428-y
Management of anterior thigh injuries in soccer players: practical guide
Abstract
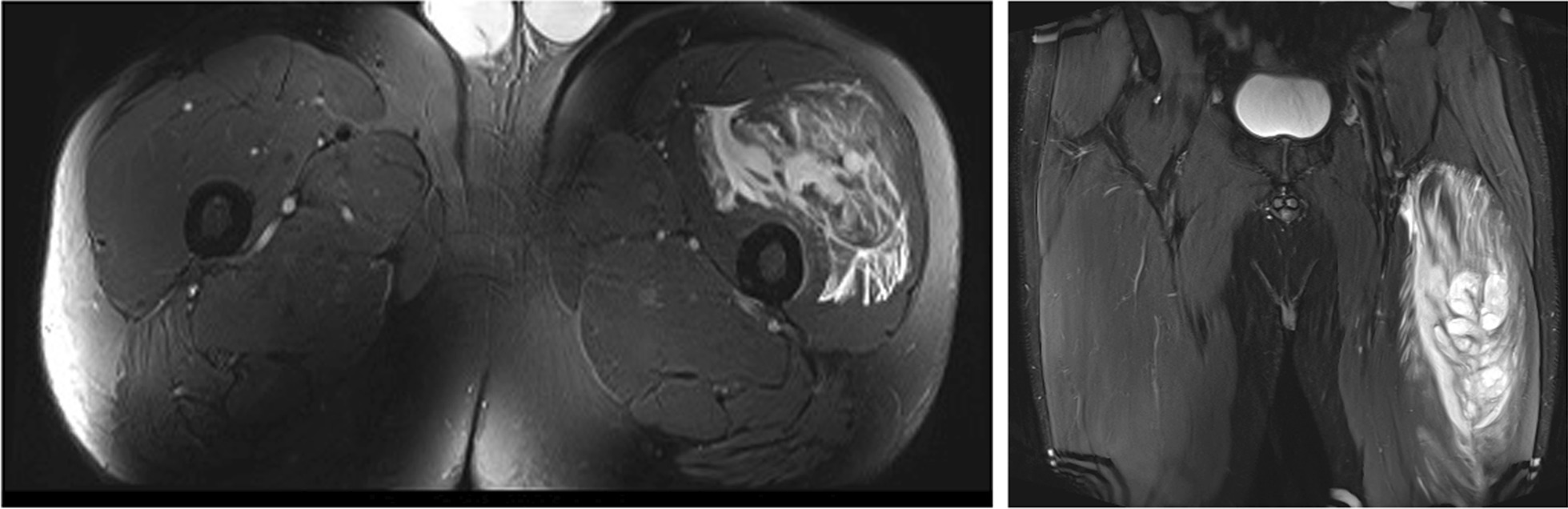
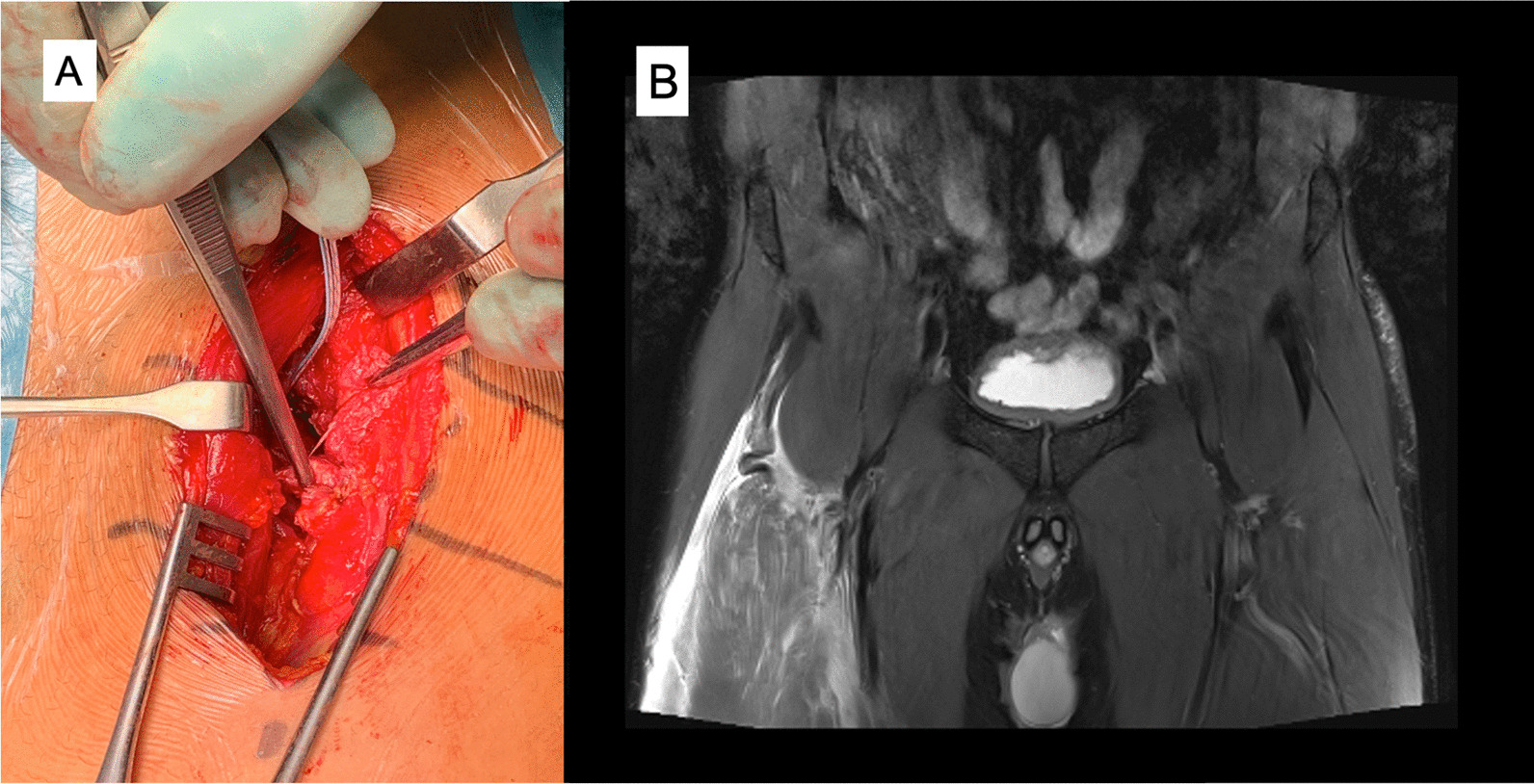
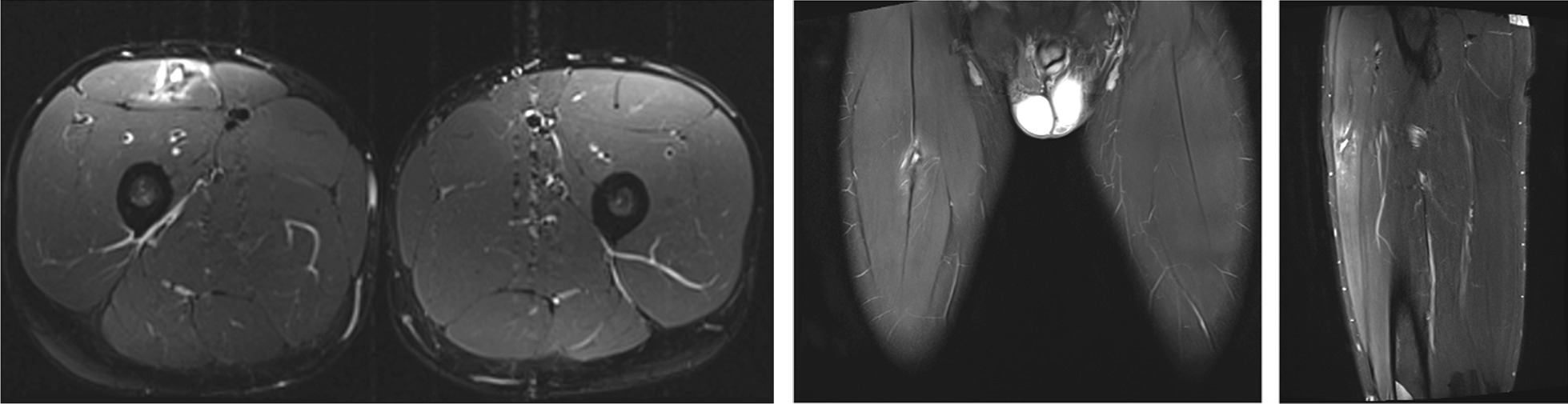
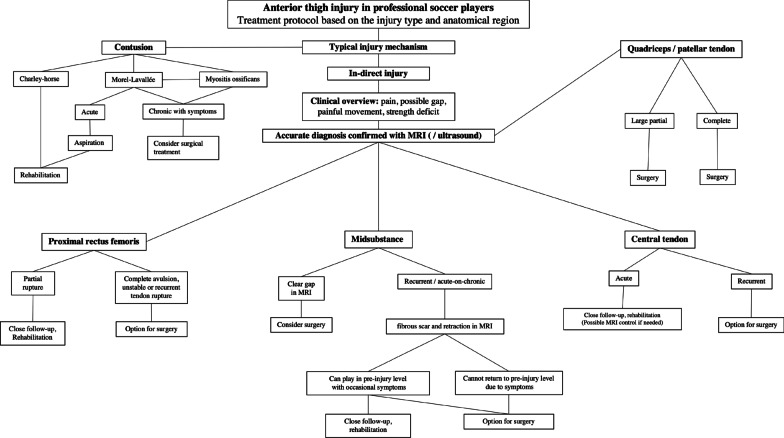
Most of the anterior thigh injuries are contusions or strains, however, some of these injuries can be career ending. Early diagnosis and correct treatment are key to successful outcome. Analyzing injury mechanism and adding both clinical and imaging findings, clinicians can make the right treatment decisions already often in the acute phase of the injury. Low grade contusions and muscle strains are treated well with planned rehabilitation, but complete tendon injuries or avulsions can require operative treatment. Also, neglected minor injuries could lead to chronic disabilities and time lost from play. Typical clinical presentation of anterior thigh injury is swelling and pain during hip flexion or knee extension. In more severe cases a clear gap can be palpated. Imaging methods used are ultrasound and magnetic resonance imaging (MRI) which are helpful for clinicians to determine more exact the extent of injury. MRI can identify possible tendon retractions which may need surgery. Clinicians should also be aware of other traumatic lesions affecting anterior thigh area such as myositis ossificans formation. Optimal treatment should be coordinated including acute phase treatment with rest, ice, and compression together with designed return-to-play protocol. The anatomical structure involved lines the treatment pathway. This narrative review describes these more common reasons for outpatient clinical visits for anterior thigh pain and injuries among soccer players.
Keywords: Quadriceps; Rectus femoris; Rehabilitation; Rupture; Soccer; Surgery; Thigh injury.
© 2022. The Author(s).
Conflict of interest statement
The authors have no competing interest to declare that are relevant to the content of this article.
Figures





Similar articles
-
Quadriceps muscle injuries in athletes: a narrative review.Br J Radiol. 2025 May 1;98(1169):630-639. doi: 10.1093/bjr/tqaf042. Br J Radiol. 2025. PMID: 39989034 Review.
-
Relationship between anatomical injury site of rectus femoris muscle strain and time taken to return to play in Japanese professional soccer players.J Orthop Surg (Hong Kong). 2022 Sep-Dec;30(3):10225536221141786. doi: 10.1177/10225536221141786. J Orthop Surg (Hong Kong). 2022. PMID: 36548509
-
Proximal Rectus Femoris Avulsion: Ultrasonic Diagnosis and Nonoperative Management.J Athl Train. 2015 Jul;50(7):778-80. doi: 10.4085/1052-6050-50.2.13. Epub 2015 May 15. J Athl Train. 2015. PMID: 25978099 Free PMC article.
-
Imaging of rectus femoris proximal tendinopathies.Skeletal Radiol. 2016 Jul;45(7):889-97. doi: 10.1007/s00256-016-2345-3. Epub 2016 Mar 8. Skeletal Radiol. 2016. PMID: 26956398 Review.
-
Epidemiological and clinical outcome comparison of indirect ('strain') versus direct ('contusion') anterior and posterior thigh muscle injuries in male elite football players: UEFA Elite League study of 2287 thigh injuries (2001-2013).Br J Sports Med. 2015 Nov;49(22):1461-5. doi: 10.1136/bjsports-2014-094285. Epub 2015 Mar 9. Br J Sports Med. 2015. PMID: 25755277
Cited by
-
Different anatomic patterns of the indirect tendon of the rectus femoris.Surg Radiol Anat. 2024 Sep;46(9):1421-1428. doi: 10.1007/s00276-024-03411-z. Epub 2024 Jun 18. Surg Radiol Anat. 2024. PMID: 38890187 Free PMC article.
-
Ultrasound imaging in professional soccer: when is it adequate?Skeletal Radiol. 2025 Apr;54(4):669-681. doi: 10.1007/s00256-023-04551-w. Epub 2023 Dec 28. Skeletal Radiol. 2025. PMID: 38151516 Review.
-
Mitigating the Risks of Lower Extremity Injuries in Soccer: A Comprehensive Analysis of Lower Extremity Injury Rates in Soccer Between 2014 and 2023.Orthop Rev (Pavia). 2024 Aug 15;16:122315. doi: 10.52965/001c.122315. eCollection 2024. Orthop Rev (Pavia). 2024. PMID: 39156913 Free PMC article.
References
-
- Cross TM, Gibbs N, Houang MT, Cameron M. Acute quadriceps muscle strains: magnetic resonance imaging features and prognosis. Am J Sports Med. 2004;32:710–719. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
