

A comparison of utilization and short-term complications of technology-assisted versus conventional total knee arthroplasty
- PMID: 35303957
- PMCID: PMC8932132
- DOI: 10.1186/s43019-022-00143-5
A comparison of utilization and short-term complications of technology-assisted versus conventional total knee arthroplasty
Abstract
Background: While technology-assisted total knee arthroplasty (TA-TKA) improves implant positioning, whether it confers improved clinical outcomes remains inconclusive. We sought to examine national TA-TKA utilization trends and to compare outcomes between TA-TKA and unassisted TKA (U-TKA).
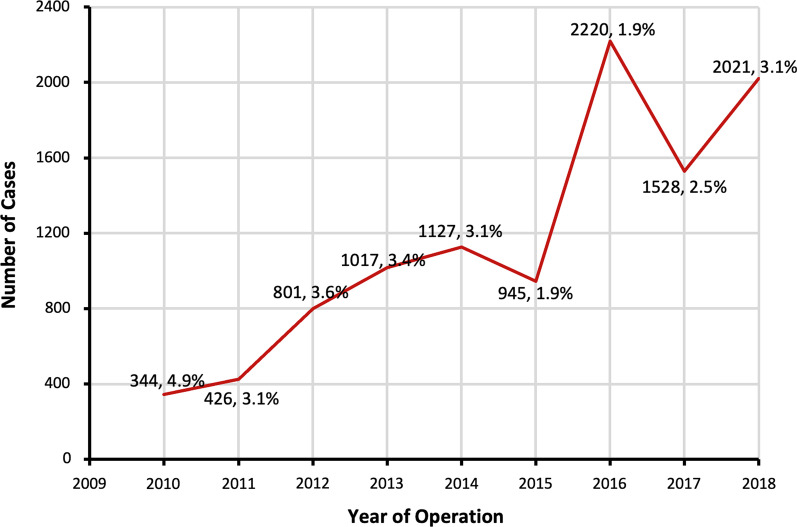
Methods: Patients who underwent primary, elective TKA from 2010 to 2018 were identified using the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database. Demographic, perioperative, and 30-day outcomes were collected. Patients were stratified on the basis of whether they underwent TA-TKA, which included computer navigation and robotics, or U-TKA. The proportion of patients undergoing TKA using TA-TKA was calculated. One-to-one propensity-score matching paired patients undergoing TA-TKA or U-TKA. Independent samples t-tests and Mann-Whitney U tests were used to compare continuous variables, and chi-squared tests were used to compare categorical variables.
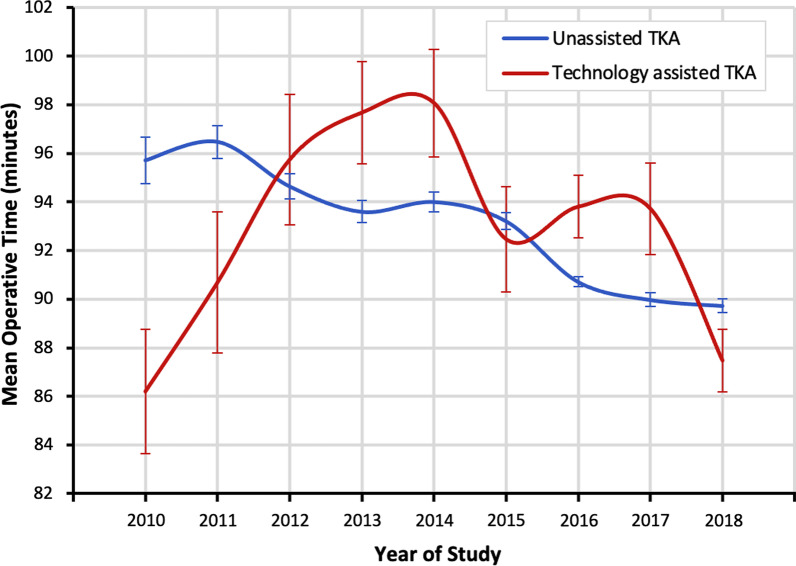
Results: Of the 402,284 TKA patients, 10,429 (2.6%) cases were performed using TA-TKA. Comparing the unmatched TA-TKA and U-TKA groups, race (p < 0.001), smoking status (p = 0.050), baseline functional status (p < 0.001), and body mass index (BMI) (p < 0.001) significantly differed. Propensity-score matching yielded 8633 TA-TKA and U-TKA pairs. The TA-TKA cohort had shorter hospital length of stay (LOS) (2.7 ± 2.5 versus 2.8 ± 1.9 days, p = 0.017) but similar operative times (92.4 ± 33.4 versus 92.6 ± 39.8 min, p = 0.670). Compared with the U-TKA group, the TA-TKA group had lower major complication (7.6% versus 9.4%, p < 0.001) and transfusion (3.9% versus 5.1%, p < 0.001) rates and higher rates of discharge to home (73.9% versus 70.4%, p < 0.001). Reoperation and readmission rates did not significantly differ between groups.
Conclusions: TA-TKA utilization remains low among orthopedic surgeons. Compared with U-TKA, TA-TKA yielded improved perioperative and 30-day outcomes. Nonetheless, surgeons must consider the benefits and drawbacks of TA-TKA when determining the proper surgical technique and technology for each patient.
Level iii evidence: Retrospective cohort study.
Keywords: Computer-assisted; Navigation; Robotics; Technology; Total knee arthroplasty.
© 2022. The Author(s).
Conflict of interest statement
R.S. reports grants and personal fees from Smith & Nephew and Intelijoint and stock or stock options from Gauss Surgical and PSI. All other authors declare that they do not have any competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
