

Federated Learning for Multicenter Collaboration in Ophthalmology: Implications for Clinical Diagnosis and Disease Epidemiology
- PMID: 35304305
- PMCID: PMC9357070
- DOI: 10.1016/j.oret.2022.03.005
Federated Learning for Multicenter Collaboration in Ophthalmology: Implications for Clinical Diagnosis and Disease Epidemiology
Abstract
Objective: To utilize a deep learning (DL) model trained via federated learning (FL), a method of collaborative training without sharing patient data, to delineate institutional differences in clinician diagnostic paradigms and disease epidemiology in retinopathy of prematurity (ROP).
Design: Evaluation of a diagnostic test or technology.
Subjects and controls: We included 5245 patients with wide-angle retinal imaging from the neonatal intensive care units of 7 institutions as part of the Imaging and Informatics in ROP study. Images were labeled with the clinical diagnoses of plus disease (plus, preplus, no plus), which were documented in the chart, and a reference standard diagnosis was determined by 3 image-based ROP graders and the clinical diagnosis.
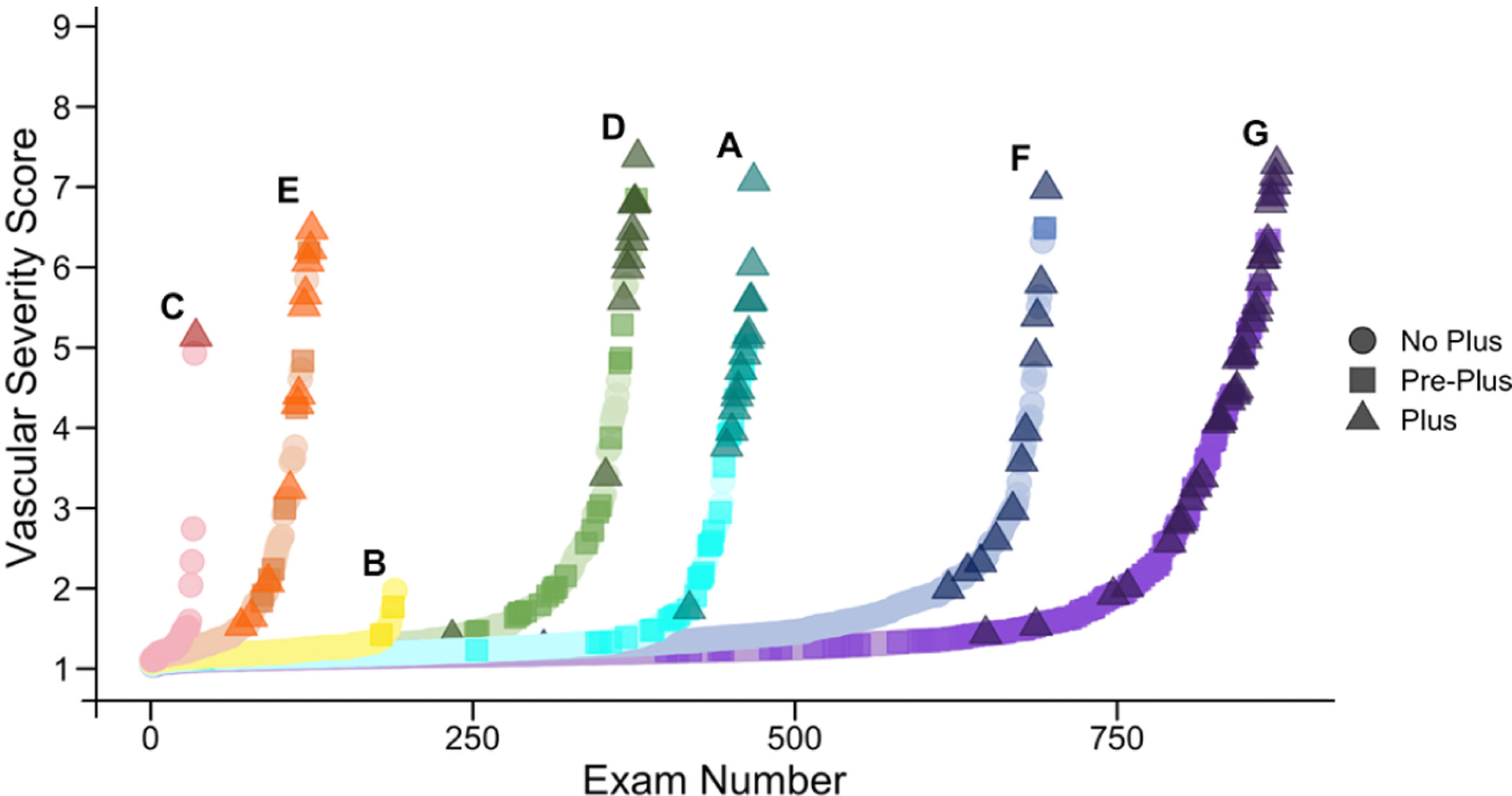
Methods: Demographics (birth weight, gestational age) and clinical diagnoses for all eye examinations were recorded from each institution. Using an FL approach, a DL model for plus disease classification was trained using only the clinical labels. The 3 class probabilities were then converted into a vascular severity score (VSS) for each eye examination, as well as an "institutional VSS," in which the average of the VSS values assigned to patients' higher severity ("worse") eyes at each examination was calculated for each institution.
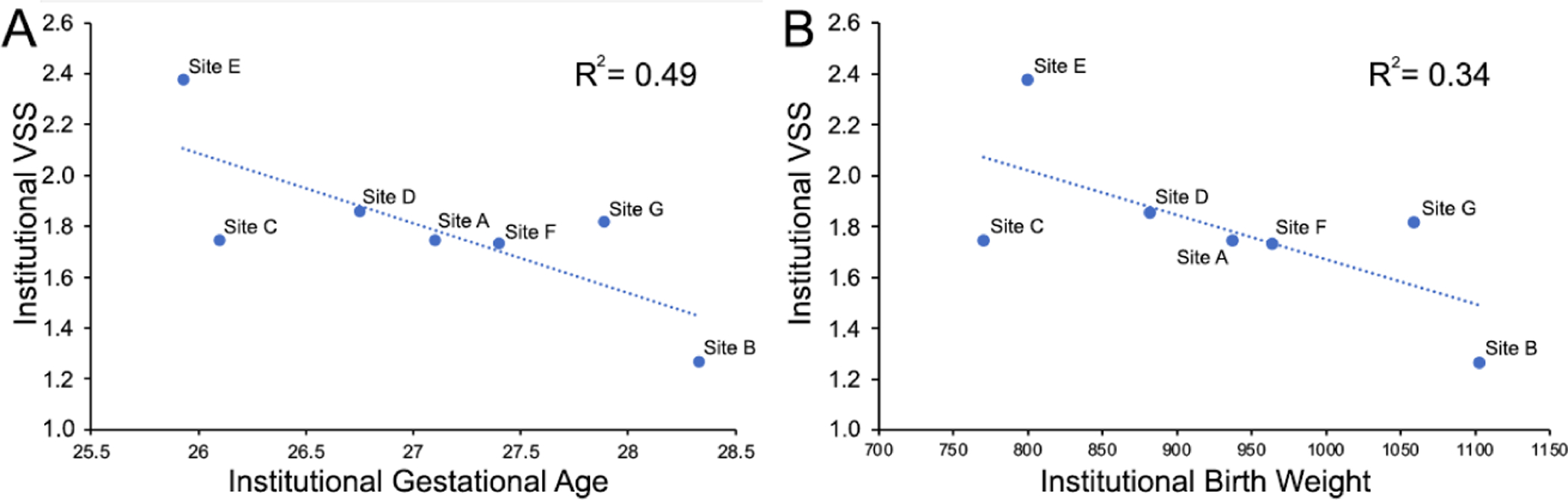
Main outcome measures: We compared demographics, clinical diagnoses of plus disease, and institutional VSSs between institutions using the McNemar-Bowker test, 2-proportion Z test, and 1-way analysis of variance with post hoc analysis by the Tukey-Kramer test. Single regression analysis was performed to explore the relationship between demographics and VSSs.
Results: We found that the proportion of patients diagnosed with preplus disease varied significantly between institutions (P < 0.001). Using the DL-derived VSS trained on the data from all institutions using FL, we observed differences in the institutional VSS and the level of vascular severity diagnosed as no plus (P < 0.001) across institutions. A significant, inverse relationship between the institutional VSS and mean gestational age was found (P = 0.049, adjusted R2 = 0.49).
Conclusions: A DL-derived ROP VSS developed without sharing data between institutions using FL identified differences in the clinical diagnoses of plus disease and overall levels of ROP severity between institutions. Federated learning may represent a method to standardize clinical diagnoses and provide objective measurements of disease for image-based diseases.
Keywords: Deep learning; Epidemiology; Federated learning; Retinopathy of prematurity.
Copyright © 2022 American Academy of Ophthalmology. All rights reserved.
Figures


Comment in
-
Federated Learning in Ophthalmology: Retinopathy of Prematurity.Ophthalmol Retina. 2022 Aug;6(8):647-649. doi: 10.1016/j.oret.2022.03.019. Ophthalmol Retina. 2022. PMID: 35933119 No abstract available.
References
-
- Reynolds JD, Dobson V, Quinn GE, et al. Evidence-based screening criteria for retinopathy of prematurity: natural history data from the CRYO-ROP and LIGHT-ROP studies. Arch Ophthalmol. 2002;120:1470–1476. - PubMed
-
- Slidsborg C, Forman JL, Fielder AR, et al. Experts do not agree when to treat retinopathy of prematurity based on plus disease. Br J Ophthalmol. 2012;96:549–553. - PubMed
-
- Quinn GE, Ells A, Capone A Jr, et al. Analysis of Discrepancy Between Diagnostic Clinical Examination Findings and Corresponding Evaluation of Digital Images in the Telemedicine Approaches to Evaluating Acute-Phase Retinopathy of Prematurity Study. JAMA Ophthalmol. 2016;134:1263–1270. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
