

Biomarker analysis from CheckMate 214: nivolumab plus ipilimumab versus sunitinib in renal cell carcinoma
- PMID: 35304405
- PMCID: PMC8935174
- DOI: 10.1136/jitc-2021-004316
Biomarker analysis from CheckMate 214: nivolumab plus ipilimumab versus sunitinib in renal cell carcinoma
Abstract
Background: The phase 3 CheckMate 214 trial demonstrated higher response rates and improved overall survival with nivolumab plus ipilimumab versus sunitinib in first-line therapy for advanced clear-cell renal cell carcinoma (RCC). An unmet need exists to identify patients with RCC who are most likely to benefit from treatment with nivolumab plus ipilimumab.
Methods: In exploratory analyses, pretreatment levels of programmed death ligand 1 were assessed by immunohistochemistry. Genomic and transcriptomic biomarkers (including tumor mutational burden and gene expression signatures) were also investigated.
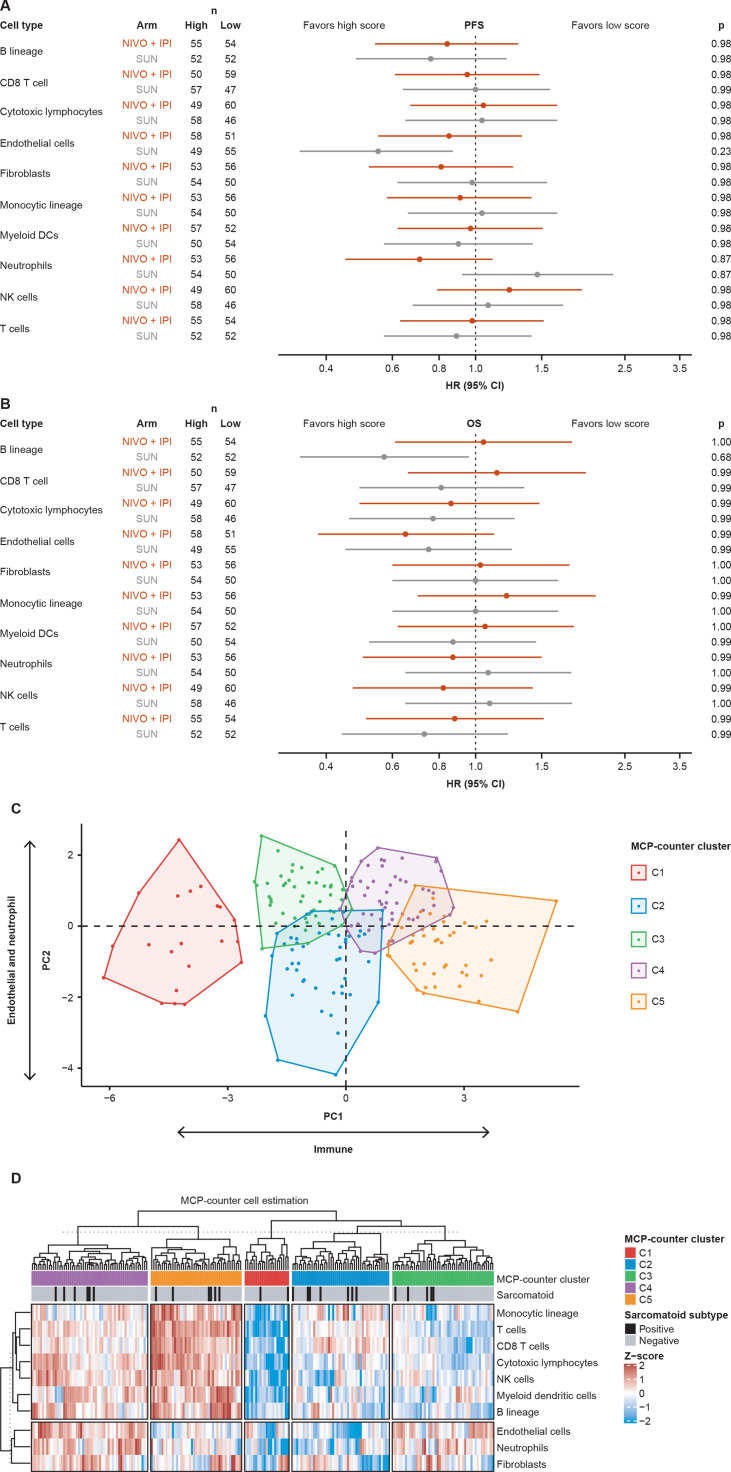
Results: Biomarkers previously associated with benefit from immune checkpoint inhibitor-containing regimens in RCC were not predictive for survival in patients with RCC treated with nivolumab plus ipilimumab. Analysis of gene expression identified an association between an inflammatory response and progression-free survival with nivolumab plus ipilimumab.
Conclusions: The exploratory analyses reveal relationships between molecular biomarkers and provide supportive data on how the inflammation status of the tumor microenvironment may be important for identifying predictive biomarkers of response and survival with combination immunotherapy in patients with RCC. Further validation may help to provide biomarker-driven precision treatment for patients with RCC.
Keywords: gene expression profiling; immunotherapy; inflammation; kidney neoplasms; tumor biomarkers.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: RJM reports consulting fees from Aveo, Calithera, Eisai, Eli Lilly, EMD Serono, Genentech, Merck, Novartis AG, Pfizer, and Roche, and contracted research to employer MSKCC for Bristol Myers Squibb, Eisai, Exelixis, Genentech, Merck, Pfizer, and Roche. TC reports personal and institutional research undertaken for Alexion, Analysis Group, AstraZeneca, Aveo, Bayer, Bristol Myers Squibb/ER Squibb & Sons LLC, Calithera, Cerulean, Corvus, Eisai, Exelixis, F. Hoffmann-La Roche, Foundation Medicine, Genentech, GlaxoSmithKline, Ipsen, Lilly, Merck, Novartis, Peloton, Pfizer, Prometheus Labs, Roche, Roche Products Limited, Sanofi/Aventis, Takeda, and Tracon; consulting/honoraria or advisory roles from Alexion, Analysis Group, AstraZeneca, Aveo, Bayer, Bristol Myers Squibb/ER Squibb & Sons LLC, Cerulean, Corvus, Eisai, EMD Serono, Exelixis, Foundation Medicine Inc, Genentech, GlaxoSmithKline, Heron Therapeutics, Infinity Pharma, Ipsen, Jansen Oncology, IQVIA, Lilly, Merck, NCCN, NiKang, Novartis, Peloton, Pfizer, Pionyr, Prometheus Labs, Roche, Sanofi/Aventis, Surface Oncology, Tempest, and Up-to-Date; travel, accommodations, expenses, and medical writing in relation to consulting, advisory roles, or honoraria; participation in CME-related events by OncLive, PVI, MJH Life Sciences, and in the NCI GU steering committee; owning Pionyr and Tempest stock; and patents filed, royalties, and other intellectual properties related to biomarkers of immune checkpoint inhibitors and ctDNA. TC is also supported in part by the Dana-Farber/Harvard Cancer Center Kidney SPORE and Program, the Kohlberg Chair at Harvard Medical School and the Trust Family, Michael Brigham, and Loker Pinard Funds for Kidney Cancer Research at DFCI. DM reports honoraria from Alkermes, Bristol Myers Squibb, Calithera Biosciences, Eisai, Eli Lilly, EMD Serono, Iovance, Merck, Pfizer, and Werewolf Therapeutics; and research support from Alkermes Inc, Bristol Myers Squibb, Exelixis, Genentech, Merck, Pfizer, and X4 Pharma. TP reports honoraria for advisory/research boards from Astellas, AstraZeneca, Bristol Myers Squibb, Eisai, Exelixis, Incyte, Ipsen, Johnson & Johnson, Merck, Merck Serono, MSD, Novartis, Pfizer, Roche, and Seattle Genetics; institutional grants and funding from Astellas, AstraZeneca, Bristol Myers Squibb, Eisai, Exelixis, Ipsen, Johnson & Johnson, Merck, Merck Serono, MSD, Novartis, Pfizer, Roche, and Seattle Genetics; and fees for travel and accommodation expenses from AstraZeneca, Ipsen, MSD, Roche, and Pfizer. YV reports no conflicts of interest. SG is employed by, and owns stock in, Bristol Myers Squibb. JY is employed by, and owns stock in, Bristol Myers Squibb. CH is employed by Bristol Myers Squibb. RA is employed by, and owns stock in, Bristol Myers Squibb. SP-C is employed by, and a shareholder of, Bristol Myers Squibb. SSS is employed by, and owns stock in, Bristol Myers Squibb. MBM is currently employed by BeiGene and owns stock in Bristol Myers Squibb. MW-R is currently employed by Agios Pharmaceuticals and owns stock in Agios Pharmaceuticals and Bristol Myers Squibb. MBM, MW-R, and PR-M were employees of Bristol Myers Squibb at the time this work was conducted.
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials