

Variations in risk-adjusted outcomes following 4318 laparoscopic liver resections
- PMID: 35305075
- PMCID: PMC9324820
- DOI: 10.1002/jhbp.1141
Variations in risk-adjusted outcomes following 4318 laparoscopic liver resections
Abstract
Background/purpose: Quality measures in surgery are important to establish appropriate levels of care and to develop improvement strategies. The purpose of this study was to provide risk-adjusted outcome measures after laparoscopic liver resection (LLR).
Methods: Data from a prospective, multicenter database involving 4318 patients submitted to LLRs in 41 hospitals from an intention-to-treat approach (2014-2020) were used to analyze heterogeneity (I2 ) among centers and to develop a risk-adjustment model on outcome measures through multivariable mixed-effect models to account for confounding due to case-mix.
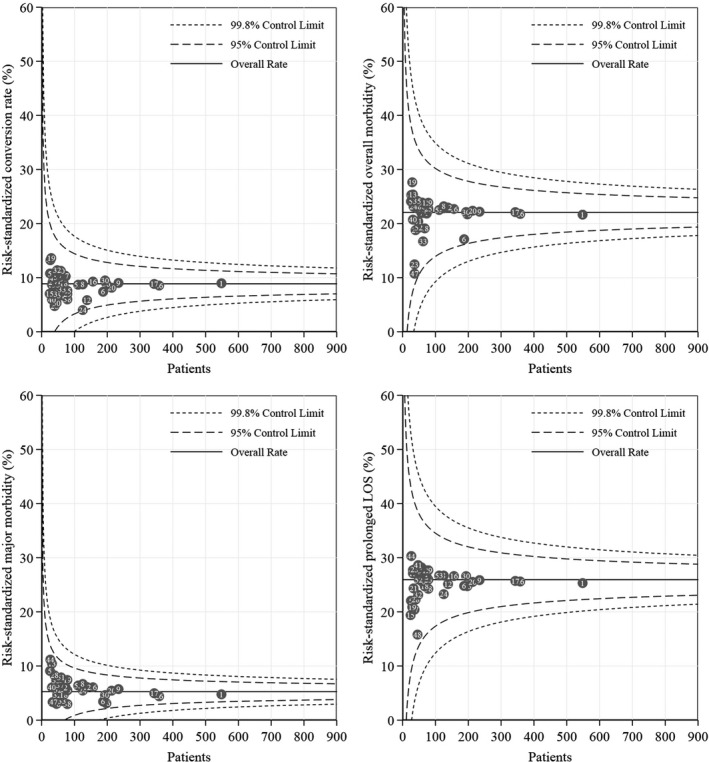
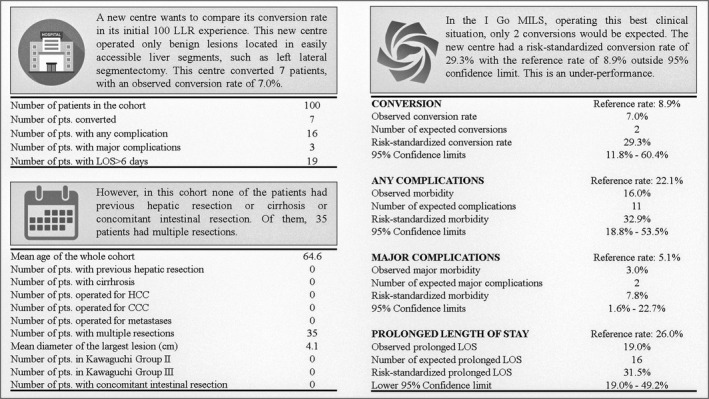
Results: Involved hospitals operated on very different patients: the largest heterogeneity was observed for operating in the presence of previous abdominal surgery (I2 :79.1%), in cirrhotic patients (I2 :89.3%) suffering from hepatocellular carcinoma (I2 :88.6%) or requiring associated intestinal resections (I2 :82.8%) and in regard to technical complexity (I2 for the most complex LLRs: 84.1%). These aspects determined substantial or large heterogeneity in overall morbidity (I2 :84.9%), in prolonged in-hospital stay (I2 :86.9%) and in conversion rate (I2 :73.4%). Major complication had medium heterogeneity (I2 :46.5%). The heterogeneity of mortality was null. Risk-adjustment accounted for all of this variability and the final risk-standardized conversion rate was 8.9%, overall morbidity was 22.1%, major morbidity was 5.1% and prolonged in-hospital stay was 26.0%. There were no outliers among the 41 participating centers. An online tool was provided.
Conclusions: A benchmark for LLRs including all eligible patients was provided, suggesting that surgeons can act accordingly in the interest of the patient, modifying their approach in relation to different indications and different experience, but finally providing the same quality of care.
Keywords: heterogeneity; laparoscopic liver resection; mortality, morbidity; risk-adjustment.
© 2022 The Authors. Journal of Hepato-Biliary-Pancreatic Sciences published by John Wiley & Sons Australia, Ltd on behalf of Japanese Society of Hepato-Biliary-Pancreatic Surgery.
Conflict of interest statement
None to declare.
Figures
References
-
- Ravaioli M, Grande G, Di Gioia P, et al. Risk avoidance and liver transplantation: a single‐center experience in a National Network. Ann Surg. 2016;264(5):778–86. - PubMed
-
- Soubrane O, Eguchi S, Uemoto S, Kwon CHD, Wakabayashi G, Han HS. Minimally invasive donor hepatectomy for adult living donor liver transplantation: an international, multi‐institutional evaluation of safety, efficacy and early outcomes. Ann Surg. 2020;275:166–74. - PubMed
-
- Nguyen KT, Gamblin TC, Geller DA. World review of laparoscopic liver resection‐2,804 patients. Ann Surg. 2009;250(5):831–41. - PubMed
-
- Cherqui D. Evolution of laparoscopic liver resection. Br J Surg. 2016;103(11):1405–7. - PubMed
-
- Aldrighetti L, Ratti F, Cillo U, et al. Diffusion, outcomes and implementation of minimally invasive liver surgery: a snapshot from the I go MILS (Italian Group of Minimally Invasive Liver Surgery) registry. Updates Surg. 2017;69(3):271–83. - PubMed
