

Severe Traumatic Brain Injury in children-paradigm of decompressive craniectomy compared to a historic cohort
- PMID: 35305153
- PMCID: PMC9061678
- DOI: 10.1007/s00701-022-05171-4
Severe Traumatic Brain Injury in children-paradigm of decompressive craniectomy compared to a historic cohort
Abstract
Purpose: Traumatic brain injury (TBI) is one of the leading causes of death and disability in children. Medical therapy remains limited, and decompressive craniectomy (DC) is an established rescue therapy in case of elevated intracranial pressure (ICP). Much discussion deals with clinical outcome after severe TBI treated with DC, while data on the pediatric population is rare. We report our experience of treating severe TBI in two different treatment setups at the same academic institution.
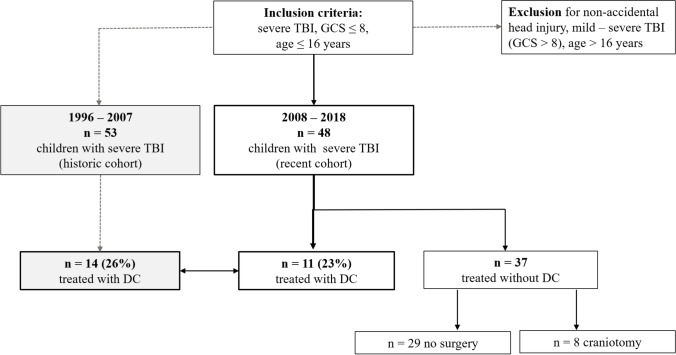
Methods: Forty-eight patients (≤ 16 years) were hospitalized with severe TBI (GCS ≤ 8 points) between 2008 and 2018 in a pediatric intensive care unit (ICU) at a specialized tertiary pediatric care center. Data on treatment, clinical status, and outcome was retrospectively analyzed. Outcome data included Glasgow Outcome Scale (GOS) at 3-, 12-, and 36-month follow-up. Data was compared to a historic cohort with 53 pediatric severe TBI patients treated at the same institution in a neurointensive care unit between 1996 and 2007. Ethical approval was granted (EA2/076/21).
Results: Between 2008 and 2018, 11 patients were treated with DC. Compared to the historic cohort, patients were younger and GCS was worse, while in-hospital mortality and clinical outcome remained similar. A trend towards more aggressive EVD placement and the internal paradigm change for treatment in a specialized pediatric ICU was observed.
Conclusions: In children with severe TBI treated over two decades, clinical outcome was comparable and mostly favorable in two different treatment setups. Consequent therapy is warranted to maintain the positive potential for favorable outcome in children with severe TBI.
Keywords: Decompressive craniectomy; Glasgow outcome score; Intracranial pressure; Pediatric traumatic brain injury; Severe TBI.
© 2022. The Author(s).
Figures


References
-
- Aldrich EF, Eisenberg HM, Saydjari C, Luerssen TG, Foulkes MA, Jane JA, Marshall LF, Marmarou A, Young HF (1992) Diffuse brain swelling in severely head-injured children. A report from the NIH Traumatic Coma Data Bank. J Neurosurg 76(3):450–454. 10.3171/jns.1992.76.3.0450 - PubMed
-
- Ballestero MFM, Furlanetti LL, Augusto LP, Chaves PHC, Santos MV, de Oliveira RS. Decompressive craniectomy for severe traumatic brain injury in children: analysis of long-term neuropsychological impairment and review of the literature. Child’s Nerv Syst. 2019;35(9):1507–1515. doi: 10.1007/s00381-019-04274-1. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
