

Body Mass Index Thresholds and the Use of Bariatric Surgery in the Field of Kidney Transplantation in Germany
- PMID: 35305229
- PMCID: PMC8986752
- DOI: 10.1007/s11695-022-06000-4
Body Mass Index Thresholds and the Use of Bariatric Surgery in the Field of Kidney Transplantation in Germany
Abstract
Background: Obesity in the recipient is linked to inferior transplant outcome. Consequently, access to kidney transplantation (KT) is often restricted by body mass index (BMI) thresholds. Bariatric surgery (BS) has been established as a superior treatment for obesity compared to conservative measures, but it is unclear whether it is beneficial for patients on the waiting list.
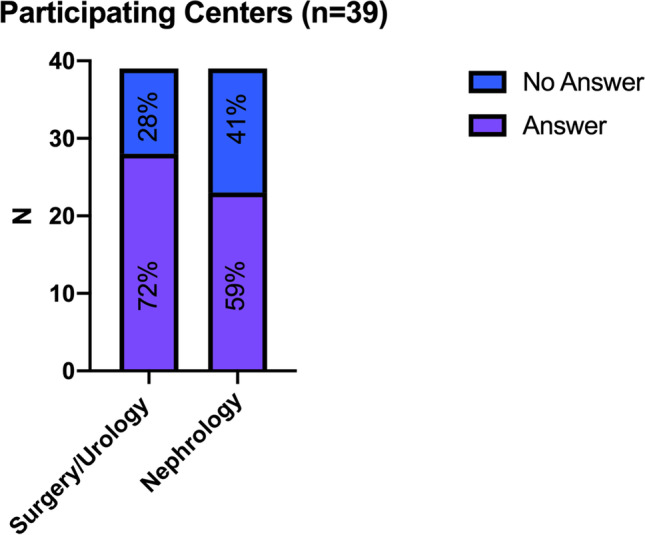
Methods: A national survey consisting of 16 questions was sent to all heads of German KT centers. Current situation of KT candidates with obesity and the status of BS were queried.
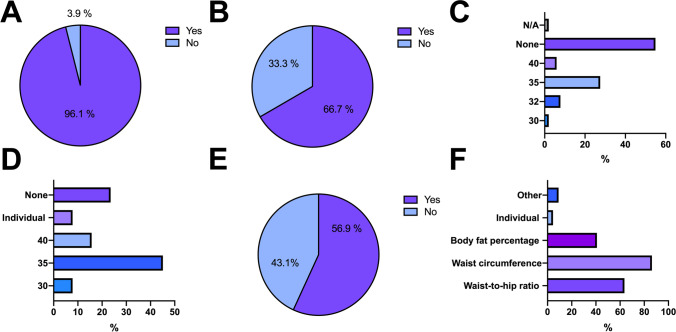
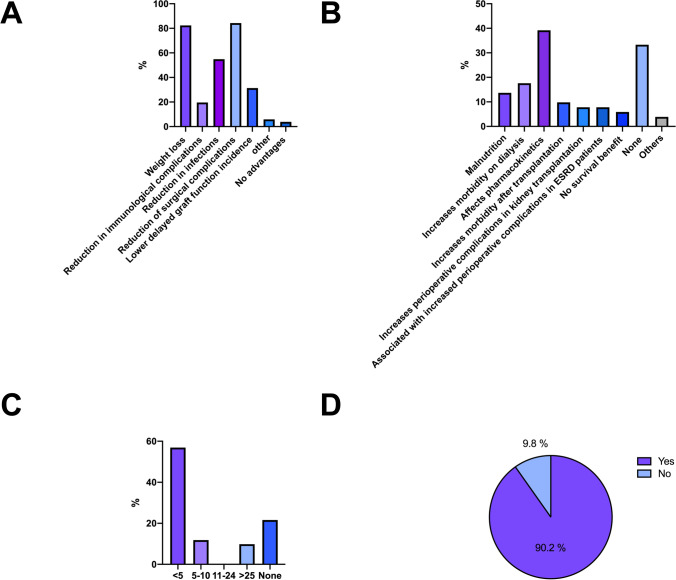
Results: Center response rate was 100%. Obesity in KT candidates was considered an important issue (96.1%; n = 49/51) and 68.6% (n = 35/51) of departments responded to use absolute BMI thresholds for KT waiting list access with ≥ 35 kg/m2 (45.1%; n = 23/51) as the most common threshold. BS was considered an appropriate weight loss therapy (92.2%; n = 47/51), in particular before KT (88.2%; n = 45/51). Sleeve gastrectomy was the most favored procedure (77.1%; n = 37/51). Twenty-one (41.2%) departments responded to evaluate KT candidates with obesity by default but only 11 (21.6%) had experience with ≥ n = 5 transplants after BS. Concerns against BS were malabsorption of immunosuppressive therapy (39.2%; n = 20/51), perioperative morbidity (17.6%; n = 9/51), and malnutrition (13.7%; n = 7/51).
Conclusions: Obesity is potentially limiting access for KT. Despite commonly used BMI limits, only few German centers consider BS for obesity treatment in KT candidates by default. A national multicenter study is desired by nearly all heads of German transplant centers to prospectively assess the potentials, risks, and safety of BS in KT waitlisted patients.
Keywords: Bariatric surgery; End-stage renal disease; Kidney transplantation; Obesity.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Comment in
-
Should sleeve gastrectomy be a preoperative standard in kidney transplant waitlisted patients with a BMI of 35 kg/m2?Obes Surg. 2022 Sep;32(9):3188-3189. doi: 10.1007/s11695-022-06198-3. Epub 2022 Jul 5. Obes Surg. 2022. PMID: 35790672 No abstract available.
-
Response to Should sleeve gastrectomy be a preoperative standard in kidney transplant waitlisted patients with a BMI of 35 kg/m2.Obes Surg. 2022 Sep;32(9):3190-3191. doi: 10.1007/s11695-022-06199-2. Epub 2022 Jul 11. Obes Surg. 2022. PMID: 35819697 Free PMC article. No abstract available.
References
-
- Koch-Institut R. Übergewicht und Adipositas. https://www.rki.de/DE/Content/Gesundheitsmonitoring/Themen/Uebergewicht_.... Accessed 1 Nov 2021.
-
- Ladhani M, Craig JC, Irving M, Clayton PA, Wong G. Obesity and the risk of cardiovascular and all-cause mortality in chronic kidney disease: a systematic review and meta-analysis. Nephrol Dial Transplant. 2017;32(3):439–449. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
