

Awake prone positioning for non-intubated patients with COVID-19-related acute hypoxaemic respiratory failure: a systematic review and meta-analysis
- PMID: 35305308
- PMCID: PMC8926412
- DOI: 10.1016/S2213-2600(22)00043-1
Awake prone positioning for non-intubated patients with COVID-19-related acute hypoxaemic respiratory failure: a systematic review and meta-analysis
Abstract
Background: Awake prone positioning has been broadly utilised for non-intubated patients with COVID-19-related acute hypoxaemic respiratory failure, but the results from published randomised controlled trials (RCTs) in the past year are contradictory. We aimed to systematically synthesise the outcomes associated with awake prone positioning, and evaluate these outcomes in relevant subpopulations.
Methods: In this systematic review and meta-analysis, two independent groups of researchers searched MEDLINE, Embase, PubMed, Web of Science, Scopus, MedRxiv, BioRxiv, and ClinicalTrials.gov for RCTs and observational studies (with a control group) of awake prone positioning in patients with COVID-19-related acute hypoxaemic respiratory failure published in English from Jan 1, 2020, to Nov 8, 2021. We excluded trials that included patients intubated before or at enrolment, paediatric patients (ie, younger than 18 years), or trials that did not include the supine position in the control group. The same two independent groups screened studies, extracted the summary data from published reports, and assessed the risk of bias. We used a random-effects meta-analysis to pool individual studies. We used the Grading of Recommendations Assessment, Development, and Evaluation approach to assess the certainty and quality of the evidence. The primary outcome was the reported cumulative intubation risk across RCTs, and effect estimates were calculated as risk ratios (RR;95% CI). The analysis was primarily conducted on RCTs, and observational studies were used for sensitivity analyses. No serious adverse events associated with awake prone positioning were reported. The study protocol was prospectively registered with PROSPERO, CRD42021271285.
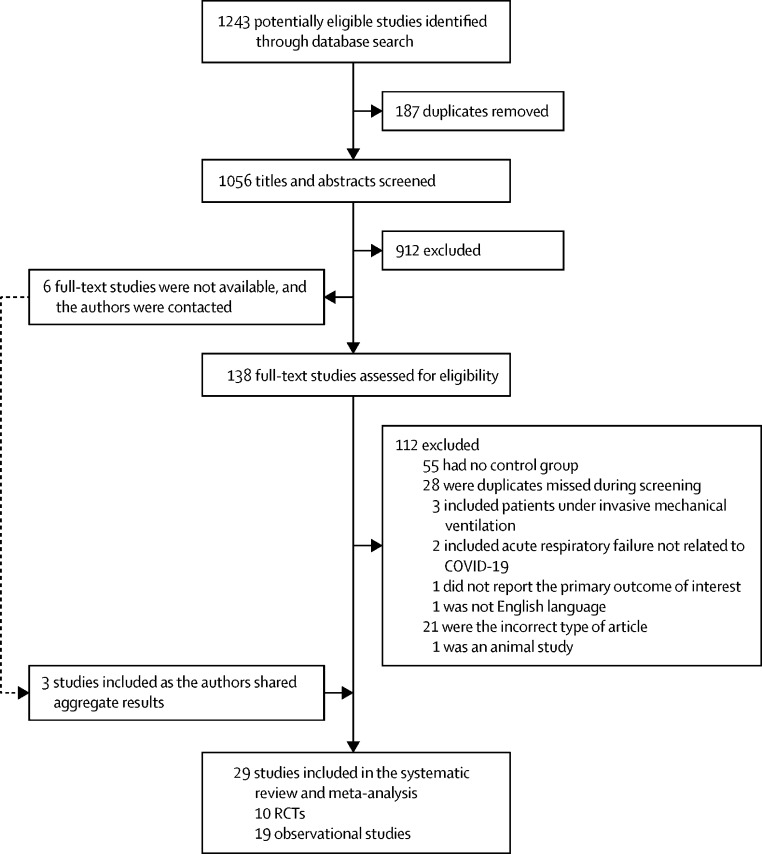
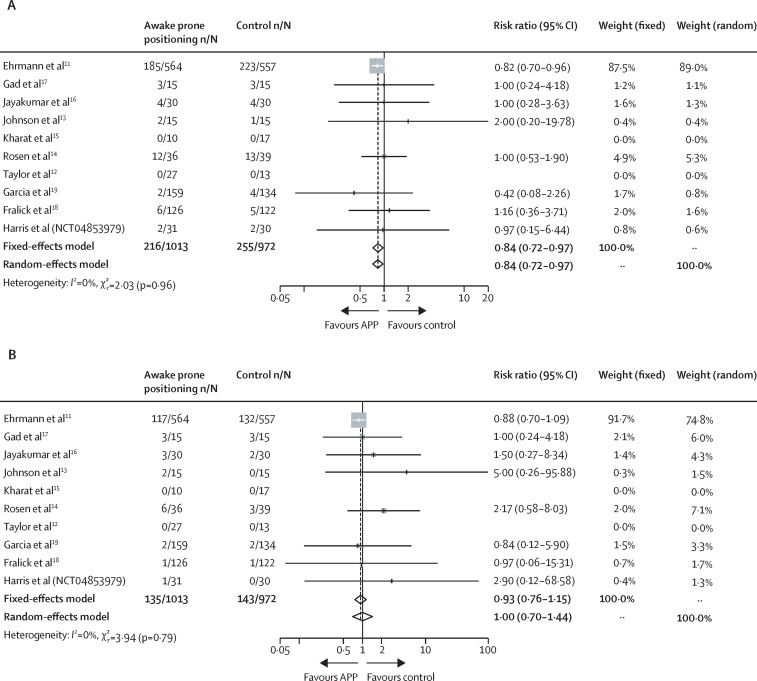
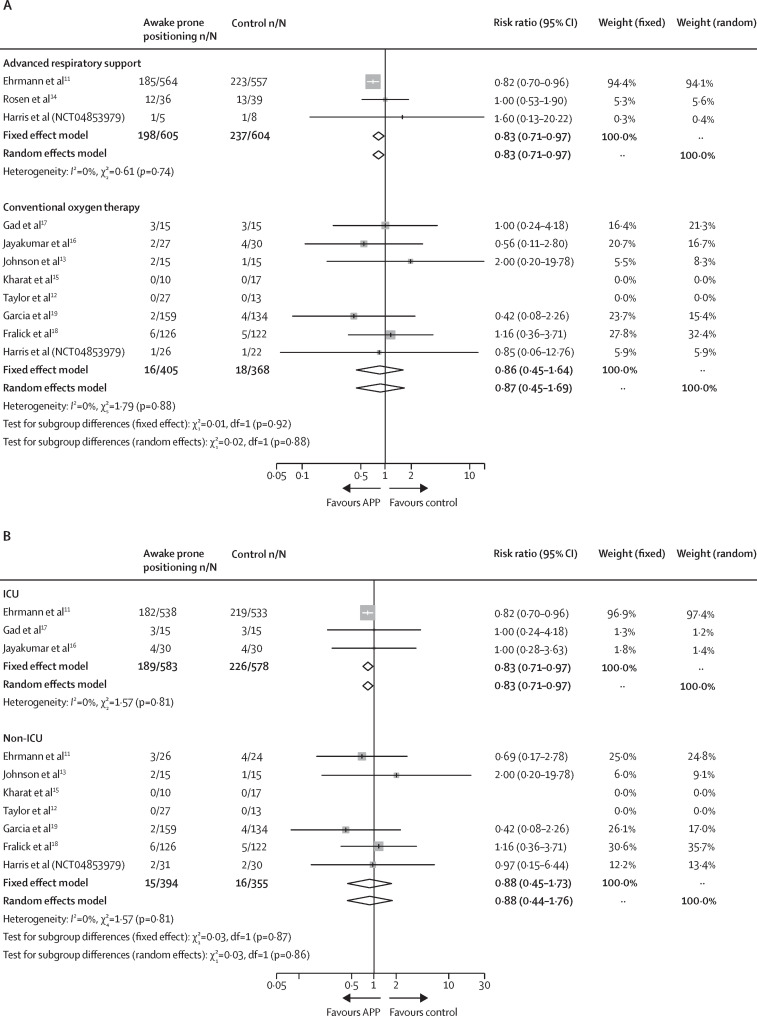
Findings: A total of 1243 studies were identified, we assessed 138 full-text articles and received the aggregated results of three unpublished RCTs; therefore, after exclusions, 29 studies were included in the study. Ten were RCTs (1985 patients) and 19 were observational studies (2669 patients). In ten RCTs, awake prone positioning compared with the supine position significantly reduced the need for intubation in the overall population (RR 0·84 [95% CI 0·72-0·97]). A reduced need for intubation was shown among patients who received advanced respiratory support (ie, high-flow nasal cannula or non-invasive ventilation) at enrolment (RR 0·83 [0·71-0·97]) and in intensive care unit (ICU) settings (RR 0·83 [0·71-0·97]) but not in patients receiving conventional oxygen therapy (RR 0·87 [0·45-1·69]) or in non-ICU settings (RR 0·88 [0·44-1·76]). No obvious risk of bias and publication bias was found among the included RCTs for the primary outcome.
Interpretation: In patients with COVID-19-related acute hypoxaemic respiratory failure, awake prone positioning reduced the need for intubation, particularly among those requiring advanced respiratory support and those in ICU settings. Awake prone positioning should be used in patients who have acute hypoxaemic respiratory failure due to COVID-19 and require advanced respiratory support or are treated in the ICU.
Funding: OpenAI, Rice Foundation, National Institute for Health Research, and Oxford Biomedical Research Centre.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SE discloses consultancy fees from Aerogen, research support from Aerogen and Fisher & Paykel Healthcare, and travel reimbursements from Aerogen and Fisher & Paykel Healthcare. JL discloses research funding from Fisher & Paykel Healthcare, Aerogen, and Rice Foundation, and speaker fees from American Association for Respiratory Care, Aerogen, Heyer, and Fisher & Paykel Healthcare. IP discloses a research grant and speaker fees from Fisher & Paykel Healthcare. YP discloses research support from Fisher & Paykel Healthcare. OR discloses a research grant from Hamilton Medical and speaker fees from Hamilton Medical, Ambu, Fisher & Paykel and Aerogen, and non-financial research support from Timpel and Masimo. DV discloses research funding from Teleflex Medical and Rice Foundation, and speaker fees from Theravance Biopharma. MT discloses consulting fees from Fisher & Paykel Healthcare. JRM discloses research support from Fisher & Paykel Healthcare, and speaker fees from Fisher & Paykel Healthcare, Gilead, Dextro and Linet. JGL discloses consulting fees from Baxter Healthcare and GlaxoSmithKline. KM is the primary investigator for the industry funded trial NCT03808922. MF is a consultant for a start-up company (ProofDx) developing a CRISPR based diagnostic test for COVID-19. All other authors declare no competing interests.
Figures
Comment in
-
The pandemic and the great awakening in the management of acute hypoxaemic respiratory failure.Lancet Respir Med. 2022 Jun;10(6):527-529. doi: 10.1016/S2213-2600(22)00051-0. Epub 2022 Mar 16. Lancet Respir Med. 2022. PMID: 35305307 Free PMC article. No abstract available.
-
Rethinking the efficacy of awake prone positioning in COVID-19-related acute hypoxaemic respiratory failure.Lancet Respir Med. 2022 Jun;10(6):e53. doi: 10.1016/S2213-2600(22)00164-3. Lancet Respir Med. 2022. PMID: 35659008 Free PMC article. No abstract available.
-
Rethinking the efficacy of awake prone positioning in COVID-19-related acute hypoxaemic respiratory failure - Authors' reply.Lancet Respir Med. 2022 Jun;10(6):e54. doi: 10.1016/S2213-2600(22)00167-9. Lancet Respir Med. 2022. PMID: 35659009 Free PMC article. No abstract available.
-
In COVID-19 acute hypoxemic respiratory failure, awake prone positioning vs. the supine position reduces intubations.Ann Intern Med. 2022 Jul;175(7):JC81. doi: 10.7326/J22-0050. Epub 2022 Jul 5. Ann Intern Med. 2022. PMID: 35785529
References
-
- Guérin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. - PubMed
-
- Scaravilli V, Grasselli G, Castagna L, et al. Prone positioning improves oxygenation in spontaneously breathing nonintubated patients with hypoxemic acute respiratory failure: a retrospective study. J Crit Care. 2015;30:1390–1394. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
