

Epidemiology, healthcare utilization, and related costs among patients with IPF: results from a German claims database analysis
- PMID: 35305632
- PMCID: PMC8933882
- DOI: 10.1186/s12931-022-01976-0
Epidemiology, healthcare utilization, and related costs among patients with IPF: results from a German claims database analysis
Abstract
Background: Idiopathic pulmonary fibrosis (IPF) is a progressive form of fibrosing interstitial pneumonia with poor survival. This study provides insight into the epidemiology, cost, and disease course of IPF in Germany.
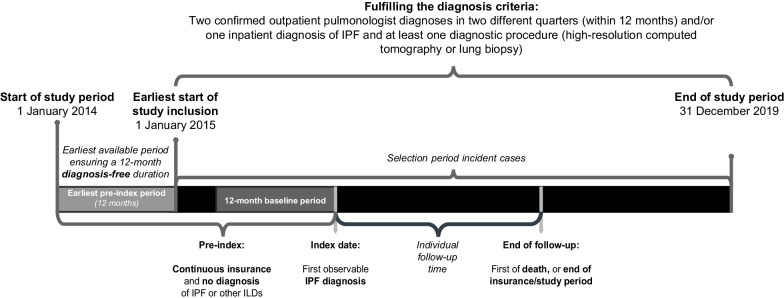
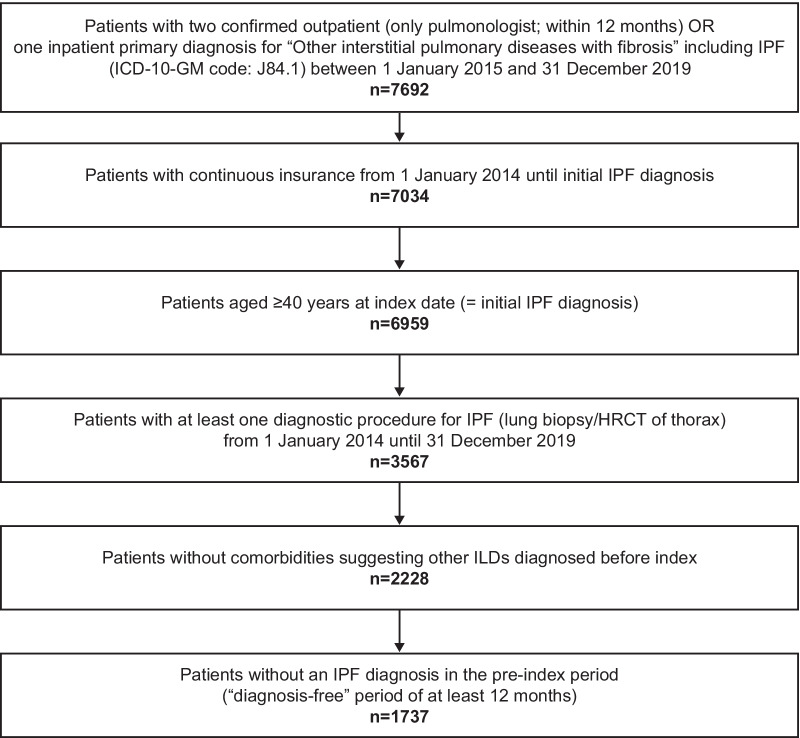
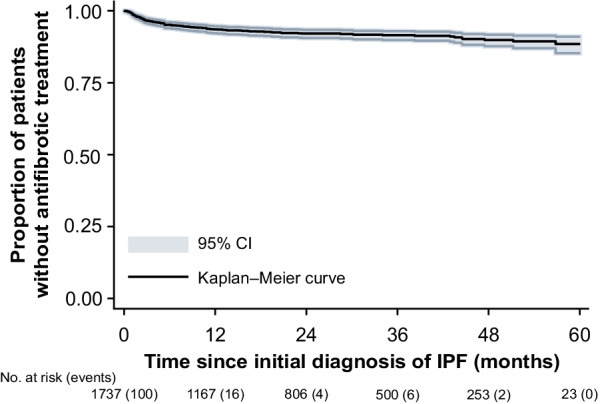
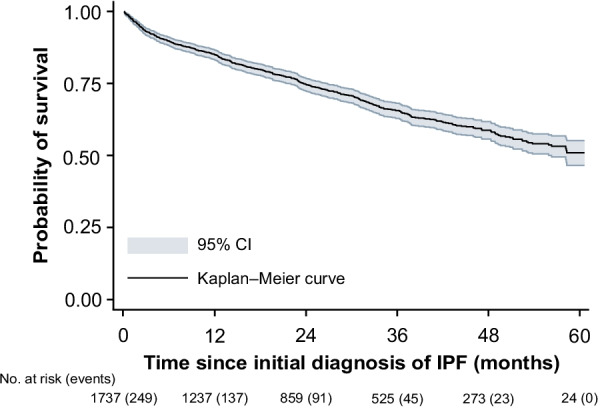
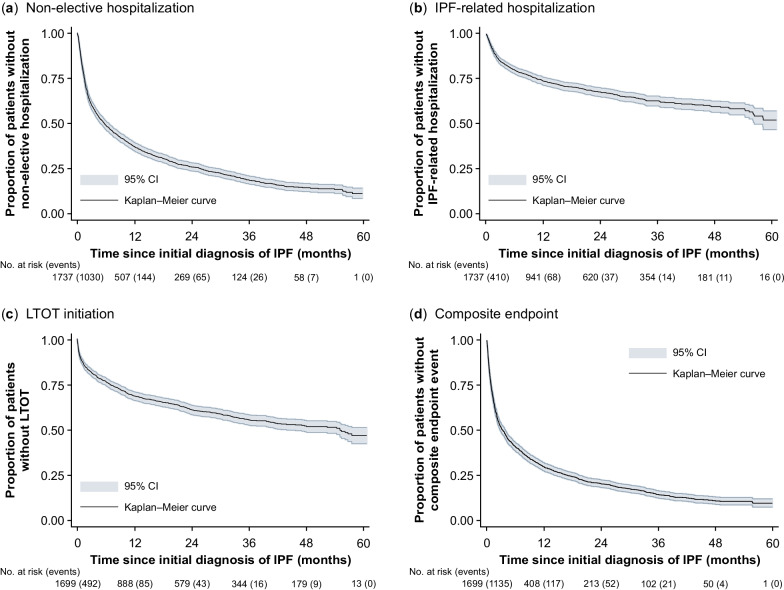
Methods: A cohort of incident patients with IPF (n = 1737) was identified from German claims data (2014-2019). Incidence and prevalence rates were calculated and adjusted for age differences compared with the overall German population. All-cause and IPF-related healthcare resource utilization as well as associated costs were evaluated per observed person-year (PY) following the initial IPF diagnosis. Finally, Kaplan-Meier analyses were performed to assess time from initial diagnosis to disease deterioration (using three proxy measures: non-elective hospitalization, IPF-related hospitalization, long-term oxygen therapy [LTOT]); antifibrotic therapy initiation; and all-cause death.
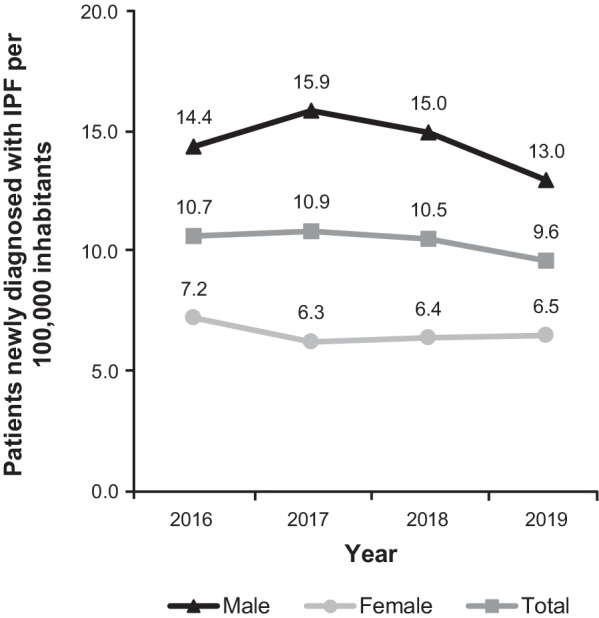
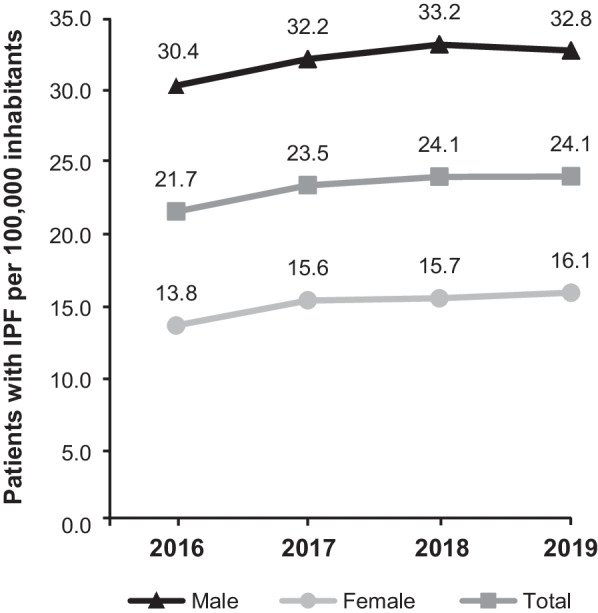
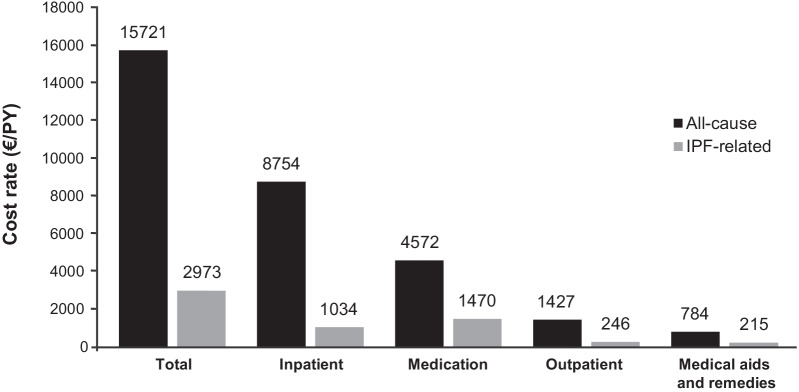
Results: The cumulative incidence of IPF was estimated at 10.7 per 100,000 individuals in 2016, 10.9 in 2017, 10.5 in 2018, and 9.6 in 2019. The point prevalence rates per 100,000 individuals for the respective years were 21.7, 23.5, 24.1, and 24.1. On average, ≥ 14 physician visits and nearly two hospitalizations per PY were observed after the initial IPF diagnosis. Of total all-cause direct costs (€15,721/PY), 55.7% (€8754/PY) were due to hospitalizations and 29.1% (€4572/PY) were due to medication. Medication accounted for 49.4% (€1470/PY) and hospitalizations for 34.8% (€1034/PY) of total IPF-related direct costs (€2973/PY). Within 2 years of the initial IPF diagnosis (23.6 months), 25% of patients died. Within 5 years of diagnosis, 53.1% of patients had initiated LTOT; only 11.6% were treated with antifibrotic agents. The median time from the initial diagnosis to the first non-elective hospitalization was 5.5 months.
Conclusion: The incidence and prevalence of IPF in Germany are at the higher end of the range reported in the literature. The main driver for all-cause cost was hospitalization. IPF-related costs were mainly driven by medication, with antifibrotic agents accounting for around one-third of the total medication costs even if not frequently prescribed. Most patients with IPF do not receive pharmacological treatment, highlighting the existing unmet medical need for effective and well-tolerated therapies.
Keywords: Claims data; Epidemiology; Healthcare costs; Healthcare resource utilization; Idiopathic pulmonary fibrosis; Incidence; Interstitial lung disease; Prevalence.
© 2022. The Author(s).
Conflict of interest statement
MK, or his institution, has received grants from Boehringer Ingelheim and Roche and remuneration for consultation by Boehringer Ingelheim, Galapagos NV, and Roche. NP and SB are employees of Ingress-Health, AD is an employee of IPAM; the work of Ingress-Health and IPAM in this study was funded by Galapagos NV. LS received consultation fees from Galapagos NV in relation to this study. UM is an employee of AOK PLUS. AC, HP, and RP are employees of Galapagos NV. JL is an employee and holds shares and warrants at Galapagos NV.
Figures
References
-
- Kreuter M, Swigris J, Pittrow D, Geier S, Klotsche J, Prasse A, et al. The clinical course of idiopathic pulmonary fibrosis and its association to quality of life over time: longitudinal data from the INSIGHTS-IPF registry. Respir Res. 2019;20(1):59. doi: 10.1186/s12931-019-1020-3. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
