

Estimated GFR Slope Across CKD Stages in Primary Hyperoxaluria Type 1
- PMID: 35306035
- PMCID: PMC9398980
- DOI: 10.1053/j.ajkd.2022.01.428
Estimated GFR Slope Across CKD Stages in Primary Hyperoxaluria Type 1
Abstract
Rationale & objective: Primary hyperoxaluria type 1 (PH1) is an autosomal recessive disorder of glyoxylate metabolism that results in early-onset kidney stone disease, nephrocalcinosis, and kidney failure. There is an unmet need for reliable markers of disease progression to test effectiveness of new treatments for patients with PH. In this study, we assessed the rate of estimated glomerular filtration rate (eGFR) decline across chronic kidney disease (CKD) glomerular filtration rate (GFR) categories (CKD G2-G5) in a cohort of patients with PH1.
Study design: Retrospective observational study.
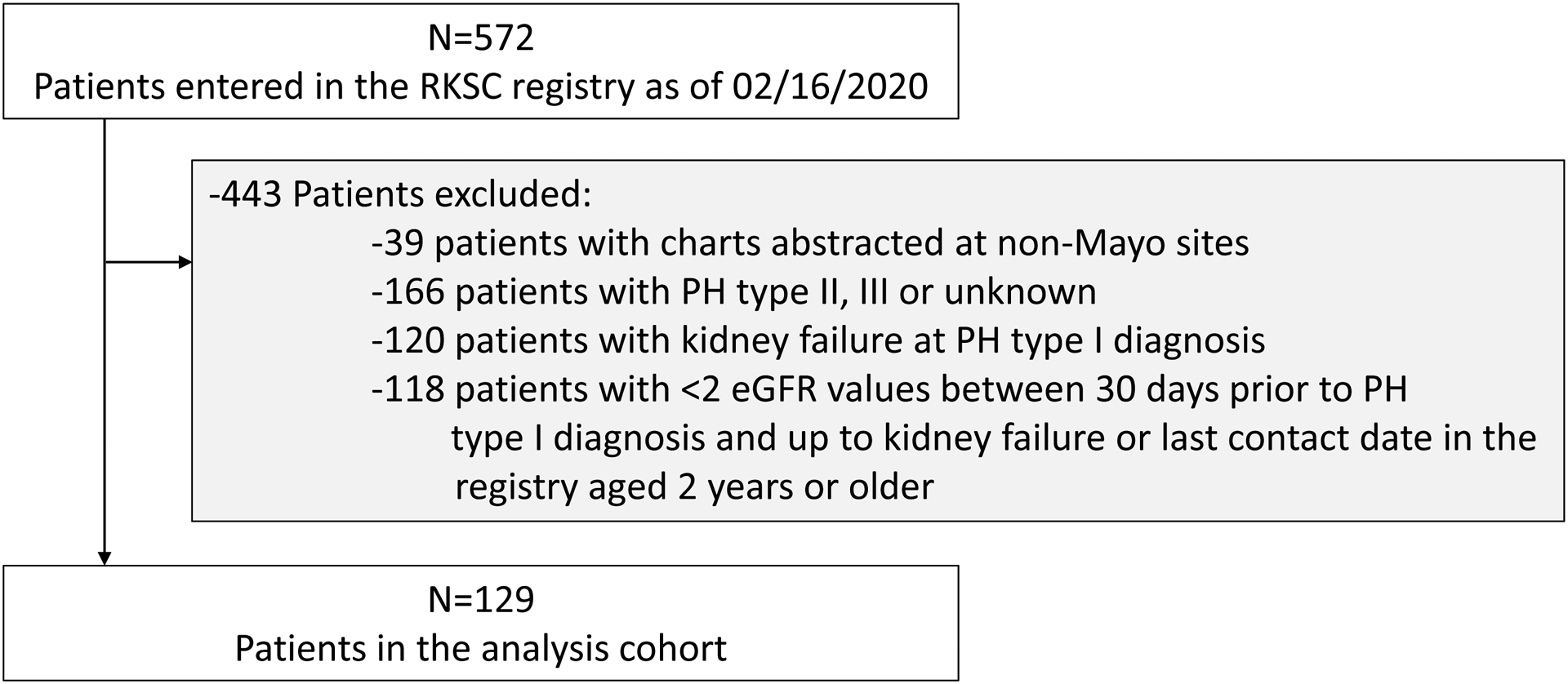
Setting & participants: Patients with PH1 enrolled in the Rare Kidney Stone Consortium (RKSC) registry who did not have kidney failure at diagnosis and who had at least 2 eGFR values recorded from within 1 month of diagnosis until their last contact date or incident kidney failure event.
Predictors: CKD GFR category, baseline patient and laboratory characteristics.
Outcome: Annualized rate of eGFR decline.
Analytical approach: Generalized estimating equations and linear regression were used to evaluate the associations between CKD GFR category, baseline patient and laboratory characteristics, and annual change in eGFR during follow-up.
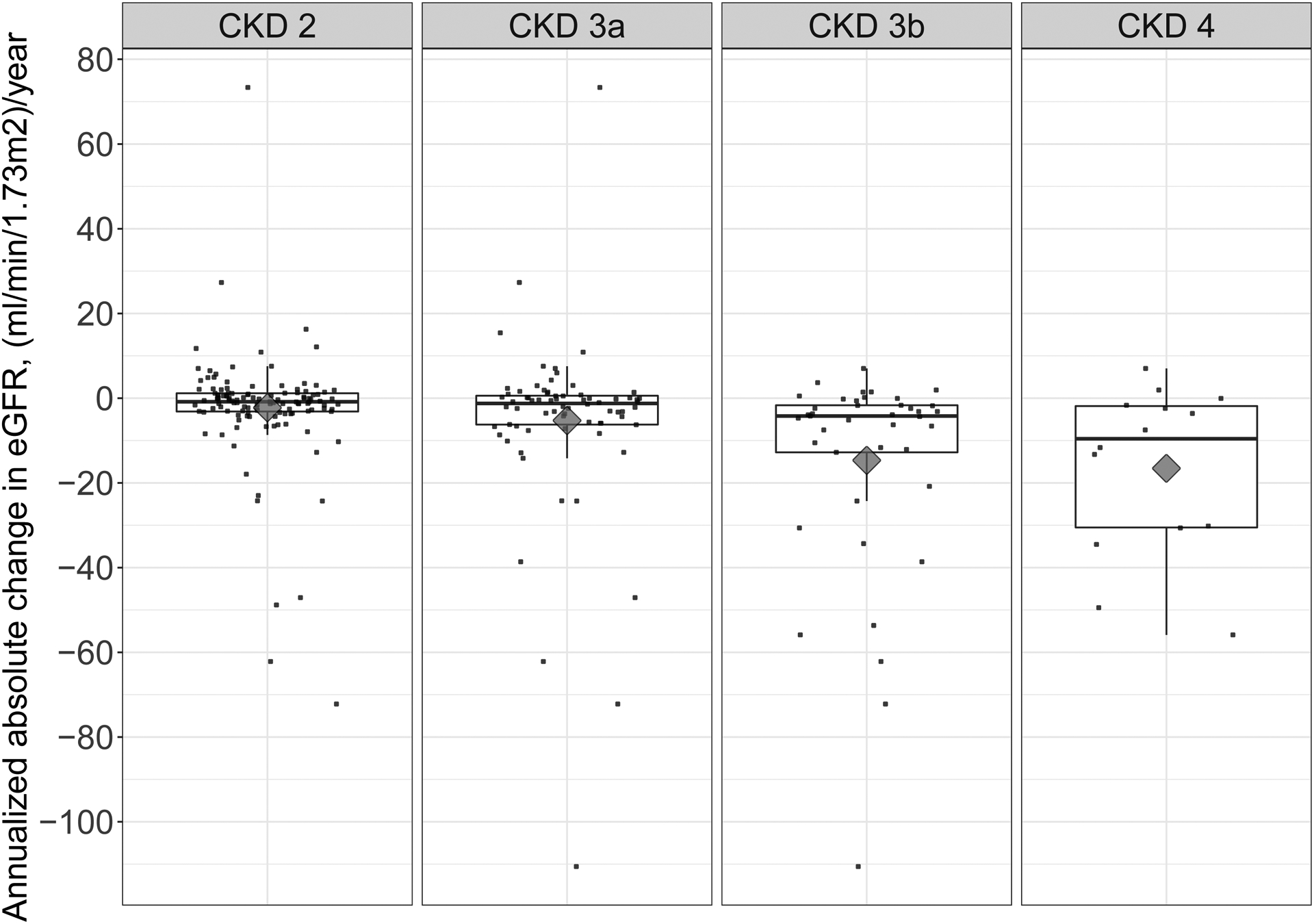
Results: Compared with the slope in CKD G2 (-2.3 mL/min/1.73 m2 per year), the mean annual eGFR decline was nominally steeper in CKD G3a (-5.3 mL/min/1.73 m2 per year) and statistically significantly more rapid in CKD G3b and G4 (-14.7 and -16.6 mL/min/1.73 m2 per year, respectively). In CKD G2, older age was associated with a more rapid rate of eGFR decline (P = 0.01). A common PH1-causing variant of alanine glyoxylate aminotransferase, a glycine to arginine substitution at amino acid 170 (G170R), appeared to be associated with less severe annual decline in eGFR.
Limitations: Data at regular time points were not available for all patients due to reliance on voluntary reporting in a retrospective rare disease registry.
Conclusions: The eGFR decline was not uniform across CKD GFR categories in this PH1 population, with a higher rate of eGFR decline in CKD G3b and G4. Thus, CKD GFR category needs to be accounted for when analyzing eGFR change in the setting of PH1.
Keywords: CKD progression; Chronic kidney disease (CKD); PH1; eGFR slope; eGFR trajectory; estimated glomerular filtration rate (eGFR); kidney failure; kidney stone; nephrocalcinosis; plasma oxalate; primary hyperoxaluria (PH); renal function; surrogate end point; urinary oxalate.
Copyright © 2022 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
