

Genetic variation within the human papillomavirus type 16 genome is associated with oropharyngeal cancer prognosis
- PMID: 35306154
- PMCID: PMC9350957
- DOI: 10.1016/j.annonc.2022.03.005
Genetic variation within the human papillomavirus type 16 genome is associated with oropharyngeal cancer prognosis
Abstract
Purpose: A significant barrier to adoption of de-escalated treatment protocols for human papillomavirus-driven oropharyngeal cancer (HPV-OPC) is that few predictors of poor prognosis exist. We conducted the first large whole-genome sequencing (WGS) study to characterize the genetic variation of the HPV type 16 (HPV16) genome and to evaluate its association with HPV-OPC patient survival.
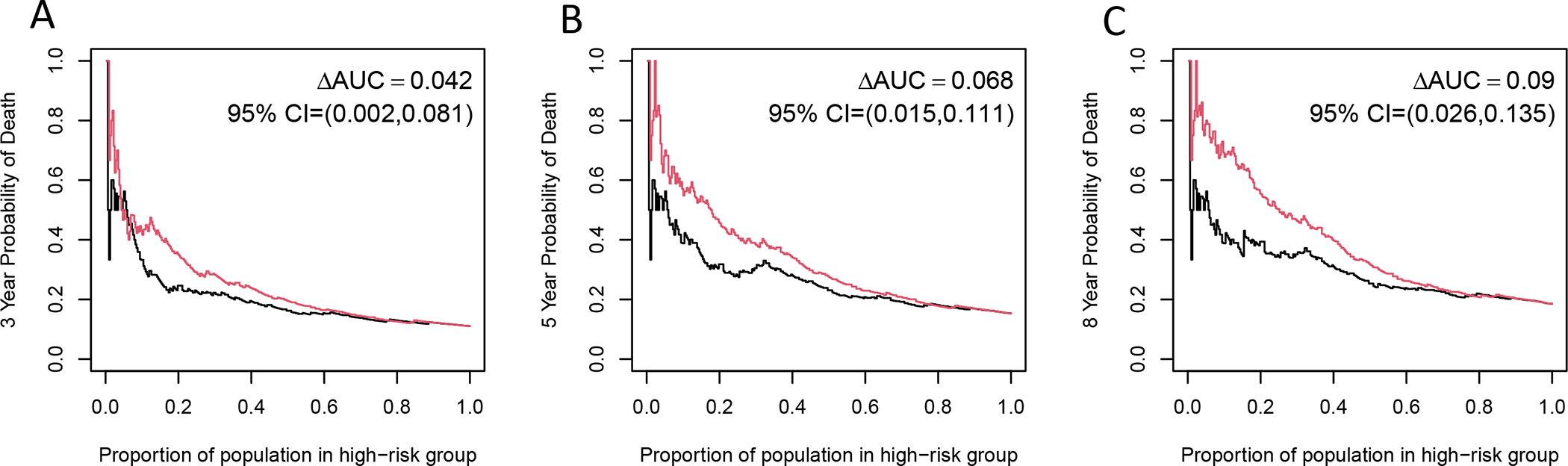
Patients and methods: A total of 460 OPC tumor specimens from two large United States medical centers (1980-2017) underwent HPV16 whole-genome sequencing. Site-specific variable positions [single nucleotide polymorphisms (SNPs)] across the HPV16 genome were identified. Cox proportional hazards model estimated hazard ratios (HRs) and 95% confidence intervals (CIs) for overall survival by HPV16 SNPs. Harrell C-index and time-dependent positive predictive value (PPV) curves and areas under the PPV curves were used to evaluate the predictive accuracy of HPV16 SNPs for overall survival.
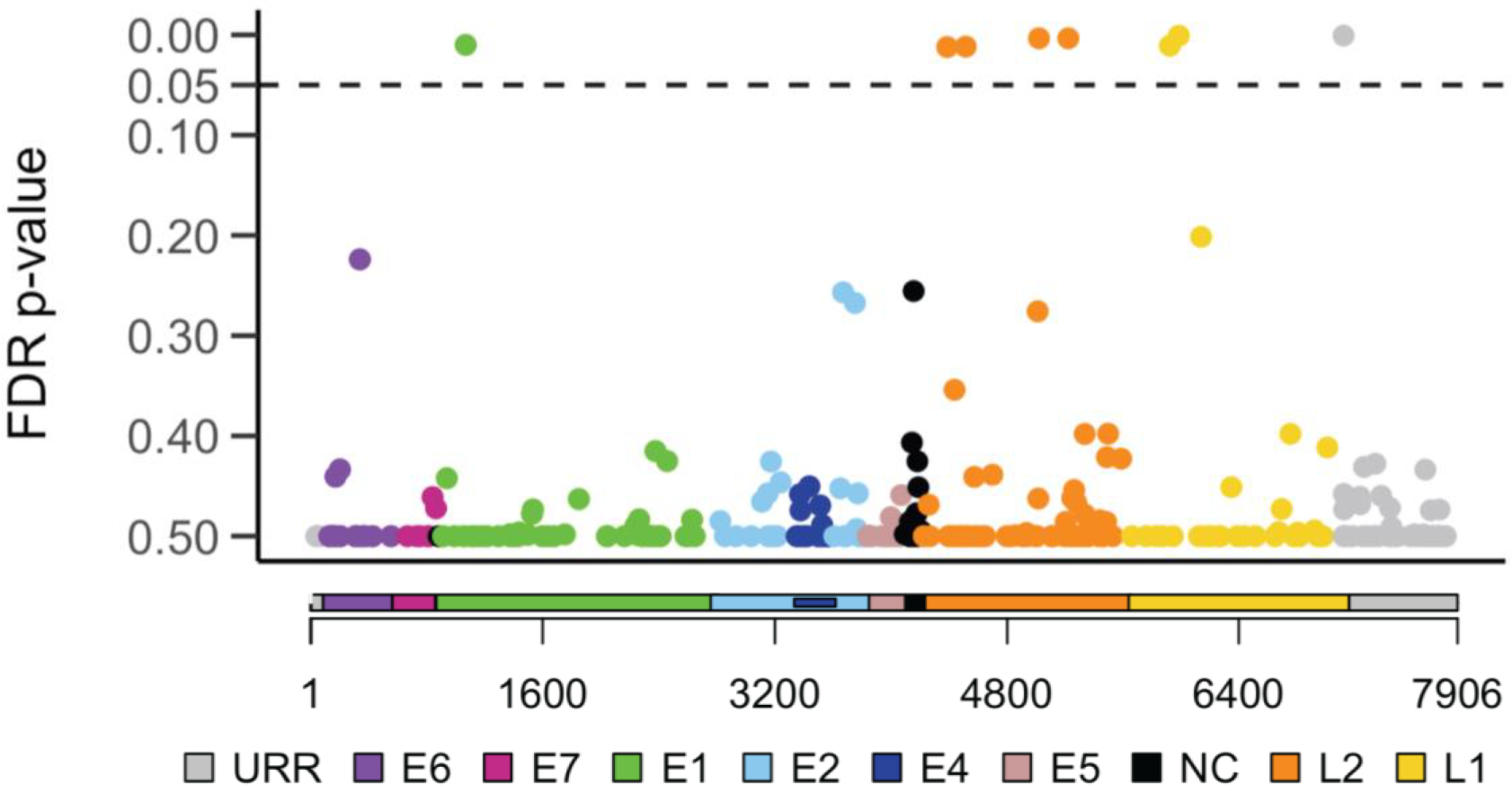
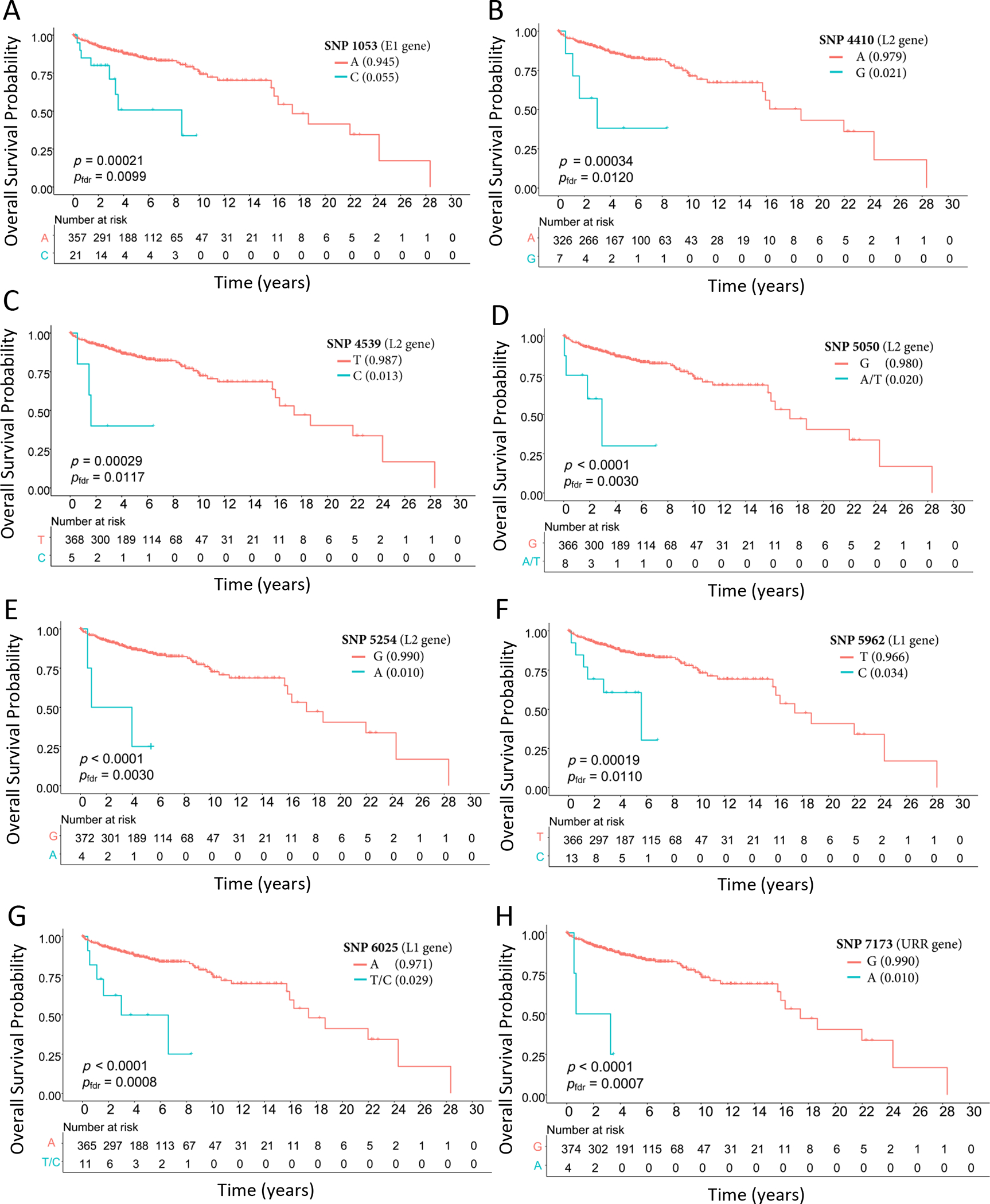
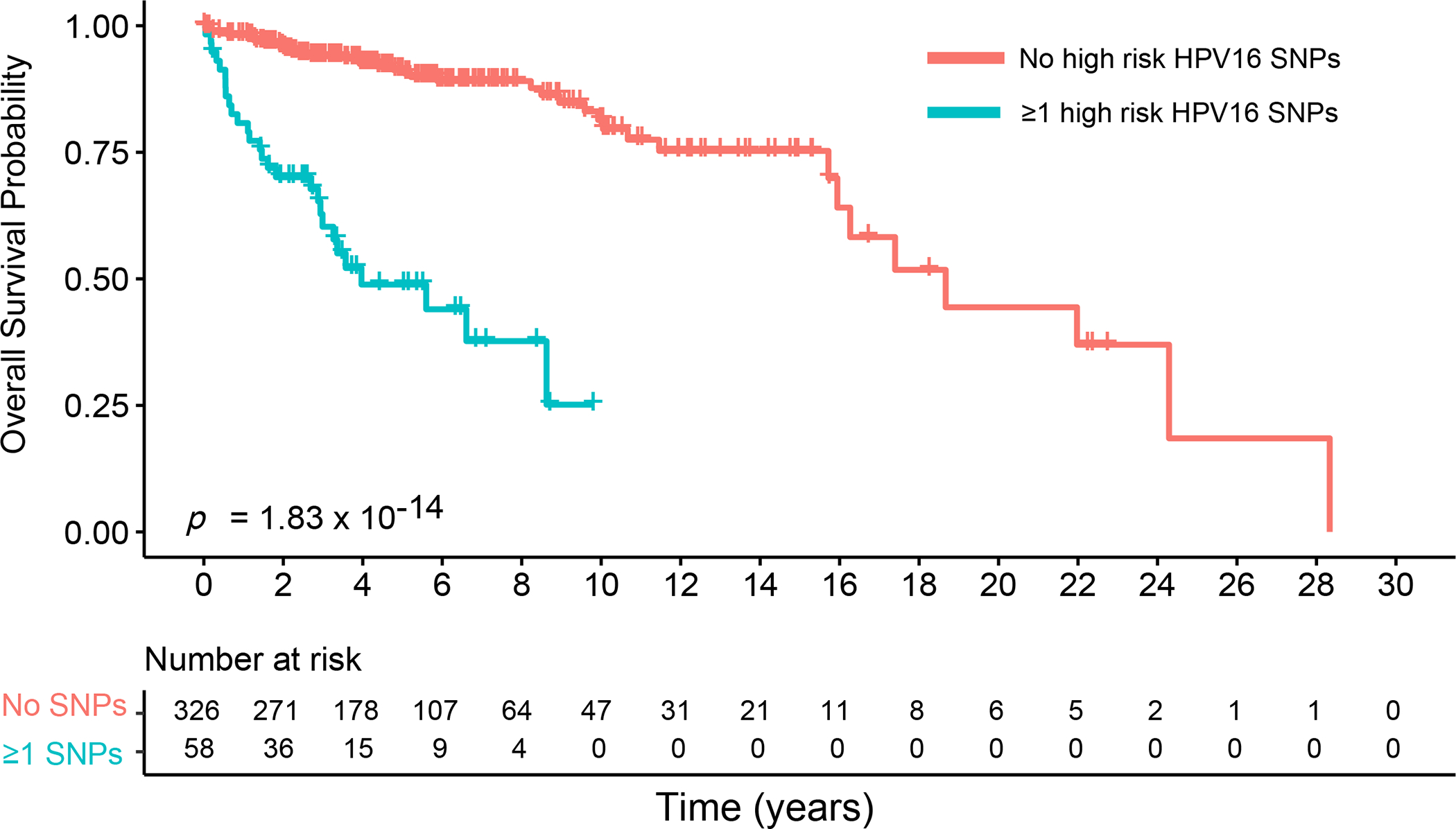
Results: A total of 384 OPC tumor specimens (83.48%) passed quality control filters with sufficient depth and coverage of HPV16 genome sequencing to be analyzed. Some 284 HPV16 SNPs with a minor allele frequency ≥1% were identified. Eight HPV16 SNPs were significantly associated with worse survival after false discovery rate correction (individual prevalence: 1.0%-5.5%; combined prevalence: 15.10%); E1 gene position 1053 [HR for overall survival (HRos): 3.75, 95% CI 1.77-7.95; Pfdr = 0.0099]; L2 gene positions 4410 (HRos: 5.32, 95% CI 1.91-14.81; Pfdr = 0.0120), 4539 (HRos: 6.54, 95% CI 2.03-21.08; Pfdr = 0.0117); 5050 (HRos: 6.53, 95% CI 2.34-18.24; Pfdr = 0.0030), and 5254 (HRos: 7.76, 95% CI 2.41-24.98; Pfdr = 0.0030); and L1 gene positions 5962 (HRos: 4.40, 95% CI 1.88-10.31; Pfdr = 0.0110) and 6025 (HRos: 5.71, 95% CI 2.43-13.41; Pfdr = 0.0008) and position 7173 within the upstream regulatory region (HRos: 9.90, 95% CI 3.05-32.12; Pfdr = 0.0007). Median survival time for patients with ≥1 high-risk HPV16 SNPs was 3.96 years compared with 18.67 years for patients without a high-risk SNP; log-rank test P < 0.001. HPV16 SNPs significantly improved the predictive accuracy for overall survival above traditional factors (age, smoking, stage, treatment); increase in C-index was 0.069 (95% CI 0.019-0.119, P < 0.001); increase in area under the PPV curve for predicting 5-year survival was 0.068 (95% CI 0.015-0.111, P = 0.008).
Conclusions: HPV16 genetic variation is associated with HPV-OPC prognosis and can improve prognostic accuracy.
Keywords: HPV16; HPV16 sublineages; HPV16 variants; OPC; oropharyngeal cancer; viral genome sequencing.
Copyright © 2022 European Society for Medical Oncology. All rights reserved.
Conflict of interest statement
Disclosure DLF has received research funding from Bristol Myers Squibb and Foundation Medicine, in-kind contributions from BostonGene, holds equity in Illumina and consulting fees from Merck, Noetic, and Focus on Boston. All other authors have declared no conflicts of interest.
Figures
References
-
- Hocking JS, Stein A, Conway EL, Regan D, Grulich A, Law M, Brotherton JM. Head and neck cancer in Australia between 1982 and 2005 show increasing incidence of potentially HPV-associated oropharyngeal cancers. British journal of cancer. 2011;104(5):886–91. Epub 2011/02/03. doi: 10.1038/sj.bjc.6606091. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
