

Relevance of cortisol and copeptin blood concentration changes in an experimental pain model
- PMID: 35306524
- PMCID: PMC8934351
- DOI: 10.1038/s41598-022-08657-4
Relevance of cortisol and copeptin blood concentration changes in an experimental pain model
Abstract
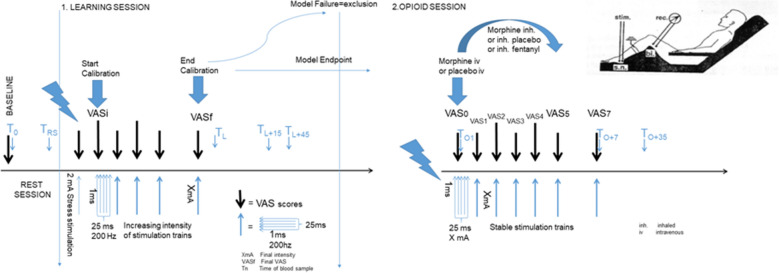
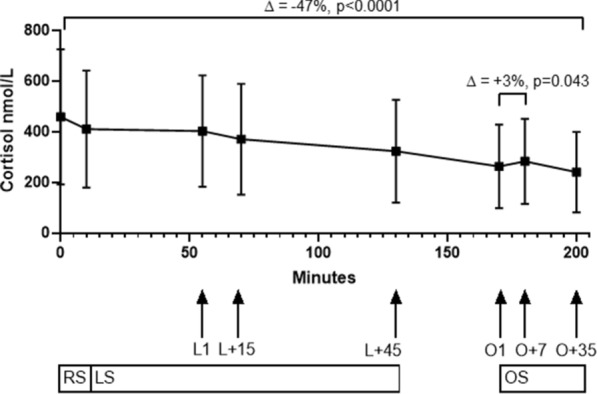
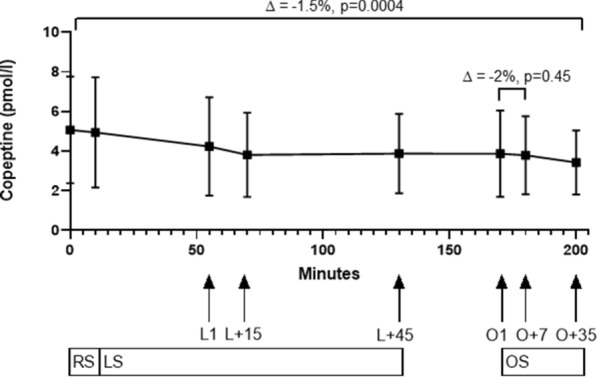
The effect of pain and analgesics on stress biomarkers is not well studied. We evaluated the effect of acute pain and analgesics on serum cortisol and copeptin in an experimental pain model in healthy volunteers. Healthy volunteers presented at 8 a.m. for an experimental pain stimulation. Cortisol and copeptin levels were measured before, during and after electrophysiological stimulation, first before and then during opioid delivery. Difference in biomarker levels compared to baseline levels was calculated, and potential influencing factors were evaluated by linear regression analysis. Cortisol decreased by 13% during the 10 min of rest at baseline, but copeptin did not change significantly. Cortisol had a median decrease of -24% or -83 nmol/l (-44 to -124 nmol/l, p = 0.0002) during the electrophysiological stimulation training session, while the median difference for copeptin was -22% or -1.01 pmol/l (-2.35 to 0.08 pmol/l, p = 0.0003). After administration of opioids, cortisol did not decrease but increased by 3% (p = 0.043), indicating an increasing opioids effect on cortisol. This effect was not visible for copeptin (median change -0.003 pmol/l (-0.50 to 0.24), p = 0.45). In this experimental pain model performed in the morning, moderate pain did not have a relevant effect on cortisol or copeptin levels, whereas opioids led to a discrete peak of cortisol.Clinicaltrials.gov identifier: NCT01975753 (registered on November 5, 2013, before start of recruitment).
© 2022. The Author(s).
Conflict of interest statement
C. A. B. received an unrestricted research grant from Novo Nordisk. ThermoFisher SA, the manufacturer of the copeptin assay, provided the assays for copeptin measurements. PH has received lectures and educational honorarium from ThermoFisher Scientific and bioMérieux unrelated to this study. All other authors have no competing interest linked to the whole trial.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
