

The Economic Burden of Insulin Injection-Induced Lipohypertophy. Role of Education: The ISTERP-3 Study
- PMID: 35306633
- PMCID: PMC9056437
- DOI: 10.1007/s12325-022-02105-5
The Economic Burden of Insulin Injection-Induced Lipohypertophy. Role of Education: The ISTERP-3 Study
Erratum in
-
Correction to: The Economic Burden of Insulin Injection-Induced Lipohypertrophy. Role of Education: The ISTERP-3 Study.Adv Ther. 2022 Jun;39(6):3058. doi: 10.1007/s12325-022-02147-9. Adv Ther. 2022. PMID: 35482252 Free PMC article. No abstract available.
Abstract
Introduction: The history of insulin-induced skin lipohypertrophy (LH) runs parallel to that of insulin's 100 years, and an average of 47% of insulin-treated patients still suffer from it today. The metabolic and economic effects of LH are significant, with hypoglycemia being the most striking. The objective of the study was to perform a 52-week follow-up of 713 insulin-treated patients with type 2 diabetes (T2DM) and LH to detect any differences in the occurrence of hypoglycemic events (HYPOs) and related healthcare costs as well as in LH rates and injection habits between an intensive education intervention group (IG) and control group (CG) provided with a single educational session at the starting point.
Methods: All participants were trained in accurately self-monitoring blood glucose and recording all HYPOs for 6 months, which allowed baseline recordings before they were randomized into the IG, comprising 395 insulin-treated subjects undergoing repeated, structured multimodal education on correct injection techniques as a longstanding behavioral rehabilitation strategy, and the CG, comprising 318 subjects receiving the same structured, multimodal educational session, but only initially.
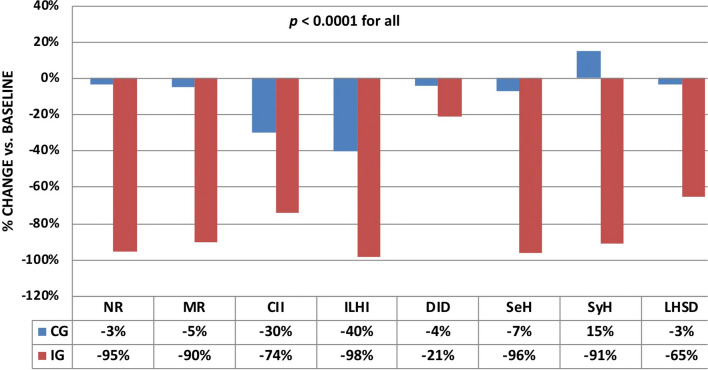
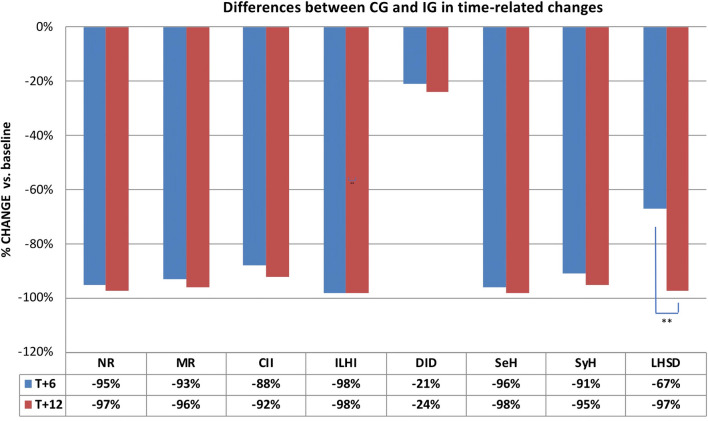
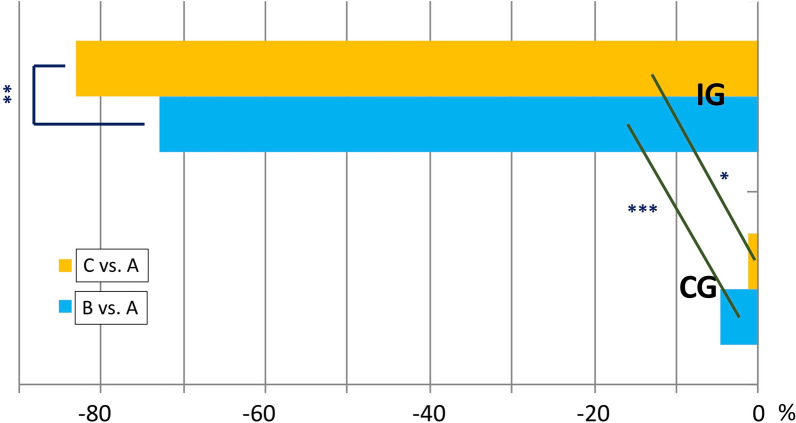
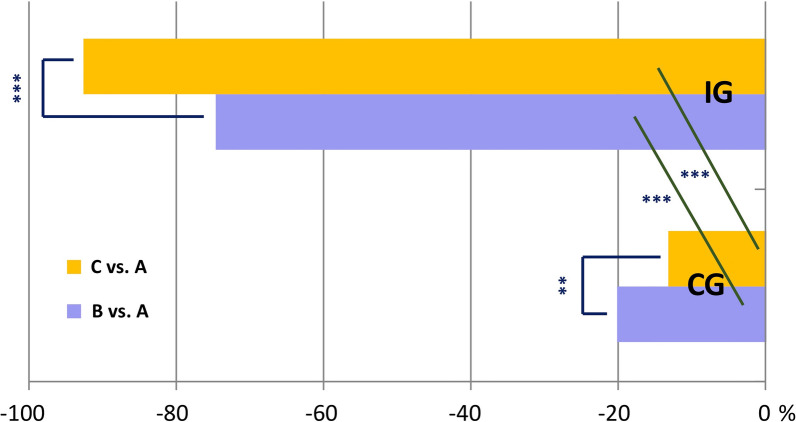
Results: Changes in LH rate and size and in performance were large in the IG and only slight and transient in the CG. A striking difference in the rate of decrease of HYPOs was also apparent between groups. Indeed, estimated costs of health interventions for severe and symptomatic HYPOs, which were on the order of €70,000 and €9300, respectively, in the two groups at baseline decreased by 5.9 times and 13.7 times, respectively, at the end of follow-up in the IG and by only approximately half in the CG. Full details of the changes occurring as a result of intensive education are provided in the text.
Conclusions: The effect of only initial education in the CG was not significant, thus providing evidence of the virtual worthlessness of a single training session on injection techniques, typical of worldwide daily clinical practice, and easily explaining the extremely high prevalence of LH in insulin-treated patients. Conversely, highly positive effects on LH prevalence and size as well as costs expected from decreased HYPO rate were obtained in the IG. To our knowledge, ours is the first 18-month randomized trial in the field. If our experimental model were to be used as an effective, longstanding behavioral rehabilitation strategy and therefore adapted to real-world settings universally, LH prevalence and costs related to their clinical consequences would be drastically reduced. However, only with a strong, relentless commitment of universities, scientific societies, and patient associations can we achieve this ambitious goal, which would provide great institutional savings and improved quality of life for people with diabetes.
Keywords: Diabetes; Economic burden; Education; Hypoglycemia; Lipohypertrophy; Rehabilitation.
© 2022. The Author(s).
Figures
References
-
- Gentile S, Guarino G, Della Corte T, et al. Role of structured education in reducing lypodistrophy and its metabolic complications in insulin-treated people with type 2 diabetes: a randomized multicenter case-control study. Diabetes Ther. 2021;12(5):1379–1398. doi: 10.1007/s13300-021-01006-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
