

When to operate after SARS-CoV-2 infection? A review on the recent consensus recommendation of the DGC/BDC and the DGAI/BDA
- PMID: 35307746
- PMCID: PMC8934603
- DOI: 10.1007/s00423-022-02495-8
When to operate after SARS-CoV-2 infection? A review on the recent consensus recommendation of the DGC/BDC and the DGAI/BDA
Abstract
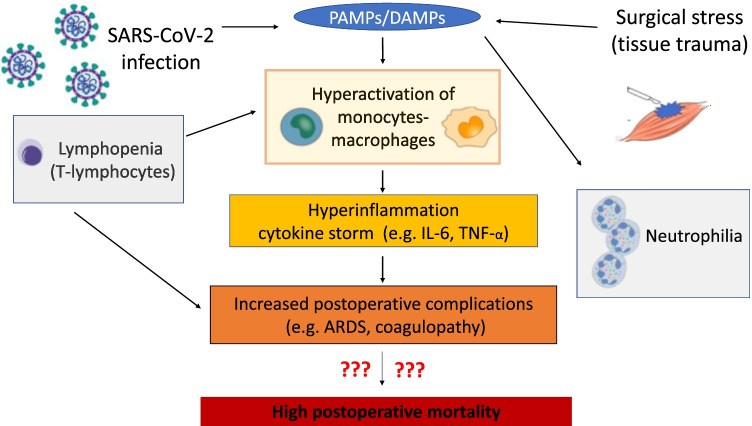
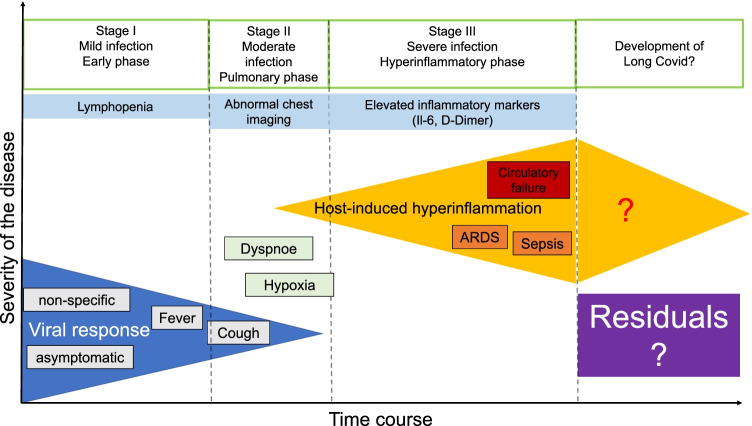
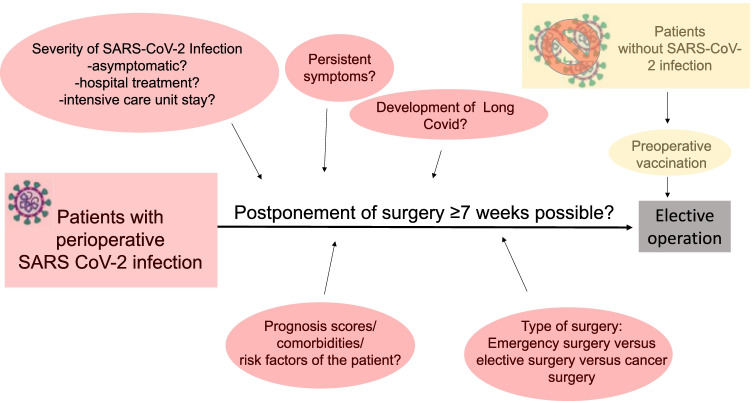
Since the eruption of the worldwide SARS-CoV-2 pandemic in late 2019/early 2020, multiple elective surgical interventions were postponed. Through pandemic measures, elective operation capacities were reduced in favour of intensive care treatment for critically ill SARS-CoV-2 patients. Although intermittent low-incidence infection rates allowed an increase in elective surgery, surgeons have to include long-term pulmonary and extrapulmonary complications of SARS-CoV-2 infections (especially "Long Covid") in their perioperative management considerations and risk assessment procedures. This review summarizes recent consensus statements and recommendations regarding the timepoint for surgical intervention after SARS-CoV-2 infection released by respective German societies and professional representatives including DGC/BDC (Germany Society of Surgery/Professional Association of German Surgeons e.V.) and DGAI/BDA (Germany Society of Anesthesiology and Intensive Care Medicine/Professional Association of German Anesthesiologists e.V.) within the scope of the recent literature. The current literature reveals that patients with pre- and perioperative SARS-CoV-2 infection have a dramatically deteriorated postoperative outcome. Thereby, perioperative mortality is mainly caused by pulmonary and thromboembolic complications. Notably, perioperative mortality decreases to normal values over time depending on the duration of SARS-CoV-2 infection.
Keywords: COVID-19; Operation; Pandemic; Postponement; SARS-CoV-2; Surgery.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
