

Characteristics and Prognostic Factors of Non-HIV Immunocompromised Patients With Pneumocystis Pneumonia Diagnosed by Metagenomics Next-Generation Sequencing
- PMID: 35308503
- PMCID: PMC8928194
- DOI: 10.3389/fmed.2022.812698
Characteristics and Prognostic Factors of Non-HIV Immunocompromised Patients With Pneumocystis Pneumonia Diagnosed by Metagenomics Next-Generation Sequencing
Abstract
Objective: The aim of this study was to evaluate the potential of metagenomic next-generation sequencing (mNGS) for the diagnosis of pneumocystis pneumonia (PCP) in patients with non-human immunodeficiency virus-infection and to discuss the clinical characteristics and identify prognostic factors associated with patients with non-HIV PCP.
Methods: Forty-six patients with PCP who were admitted in respiratory intensive care unit (ICU) between May 2018 and May 2020 were retrospectively reviewed. The subjects were divided into survivor and non-survivor groups according to the patients' outcome. Conventional methods and mNGS for detecting Pneumocystis jirovecii (P. jirovecii) were analyzed. The patients' demographics, comorbidities, laboratory parameters, and treatments were compared and evaluated in both groups to identify risk factors for mortality by using univariate and multivariate logistic regression.
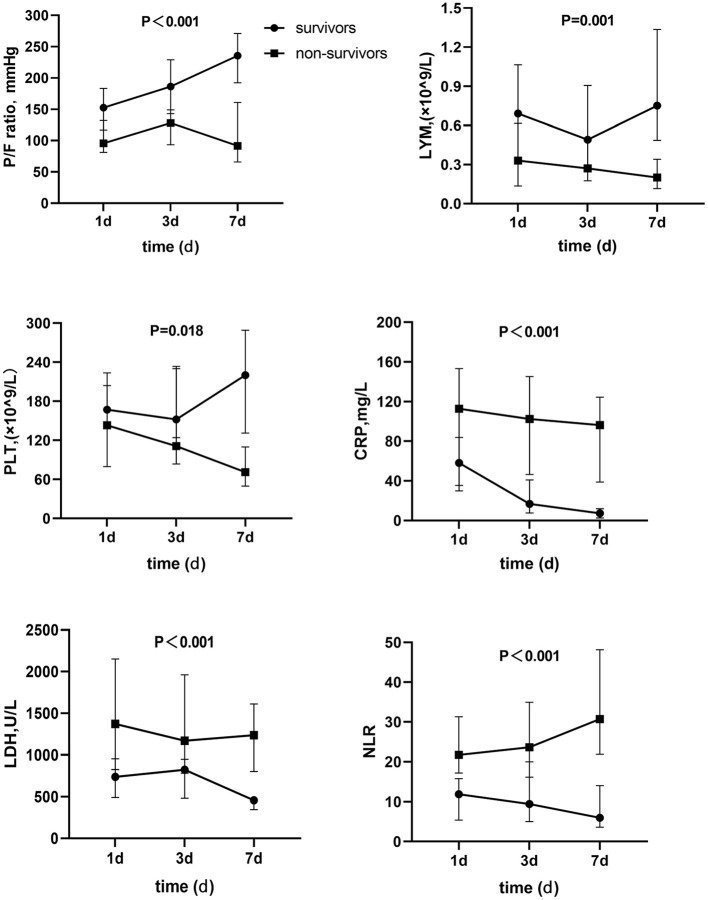
Results: Metagenomic next-generation sequencing (mNGS) showed a satisfying diagnostic performance of 100% positive of detecting P. jirovecii from bronchoalveolar lavage (BAL) specimens in forty-six patients with non-HIV PCP, compared to only 15.2% for Gomori Methenamine silver (GMS) staining and 84.8% for Serum 1,3-beta-D-glucan (BDG). Among them, the mean age was 46.4-year-old (range 18-79-year-old) and mortality rate was 43.5%. The dominant underlying conditions were connective tissue diseases (34.8%), autoimmune kidney diseases (30.4%), followed by hematologic malignancies (10.9%), and solid organ transplantation (6.5%). A total of 38 cases (82.6%) received glucocorticoid and 19 cases (41.3%) used immunosuppressant within 3 months before diagnosed PCP. Multiple infections were very common, over two thirds' cases had mixed infections. Compared with survivors, non-survivors had a higher acute physiology and chronic health evaluation II (APACHE II) score (14.4 ± 4.8 vs. 10 ± 3.4), Procalcitonin (PCT) [ng/ml: 0.737 (0.122-1.6) vs. 0.23 (0.095-0.35)], lactic dehydrogenase (LDH) [U/L: 1372 (825.5-2150) vs. 739 (490.5-956)], and neutrophil-lymphocyte ratio (NLR) [21.6 (15.67-38.2) vs. 11.75 (5.1-15.52)], but had a lower PaO2/FiO2 ratio (mmHg:108.8 ± 42.4 vs. 150.5 ± 47.5), lymphocytes [×109/L: 0.33 (0.135-0.615) vs. 0.69 (0.325-1.07)] and CD4+ T cells [cell/μl: 112 (53.5-264) vs. 255 (145-303.5)], all P < 0.05. Furthermore, we found non-survivors' PaO2/FiO2 ratio of day 3 and day 7 had not improved when compared with that of day one, and platelet level and NLR became worse. Multivariate analysis showed that other pathogens' co-infection (OR = 9.011, 95% CI was 1.052-77.161, P = 0.045) and NLR (OR = 1.283, 95% CI was 1.046-1.547, P = 0.017) were the independent risk factors of poor prognosis.
Conclusion: mNGS is a very sensitive diagnostic tool for identifying P. jirovecii in patients who are non-HIV immunocompromised. PCP in patients who are non-HIV infected is associated with a high rate of multiple infections and severe condition. Mixed infection and elevation of NLR were the independent risk factors of poor prognosis.
Keywords: Pneumocystis jirovecii; immunocompromised; mNGS; non-HIV; pneumonia.
Copyright © 2022 Duan, Gao, Liu, Sun, Liu, Tan and Xing.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Metagenomic next-generation sequencing for the diagnosis of Pneumocystis jirovecii Pneumonia in critically pediatric patients.Ann Clin Microbiol Antimicrob. 2023 Jan 16;22(1):6. doi: 10.1186/s12941-023-00555-5. Ann Clin Microbiol Antimicrob. 2023. PMID: 36647095 Free PMC article.
-
The diagnostic value of metagenomic next-generation sequencing for identifying Pneumocystis jirovecii infection in non-HIV immunocompromised patients.Front Cell Infect Microbiol. 2022 Oct 27;12:1026739. doi: 10.3389/fcimb.2022.1026739. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36389151 Free PMC article.
-
Metagenomic next-generation sequencing-based diagnosis of Pneumocystis jirovecii pneumonia in patients without human immunodeficiency virus infection: A dual-center retrospective propensity matched study.J Infect Public Health. 2025 Sep;18(9):102831. doi: 10.1016/j.jiph.2025.102831. Epub 2025 May 19. J Infect Public Health. 2025. PMID: 40472476
-
Exploring the Differences in Pneumocystis Pneumonia Infection Between HIV and Non-HIV Patients.Cureus. 2022 Aug 6;14(8):e27727. doi: 10.7759/cureus.27727. eCollection 2022 Aug. Cureus. 2022. PMID: 36106266 Free PMC article. Review.
-
Clinical, Diagnostic, and Treatment Disparities between HIV-Infected and Non-HIV-Infected Immunocompromised Patients with Pneumocystis jirovecii Pneumonia.Respiration. 2018;96(1):52-65. doi: 10.1159/000487713. Epub 2018 Apr 10. Respiration. 2018. PMID: 29635251 Review.
Cited by
-
Pneumocystis jirovecii Pneumonia after Heart Transplantation: Two Case Reports and a Review of the Literature.Pathogens. 2023 Oct 21;12(10):1265. doi: 10.3390/pathogens12101265. Pathogens. 2023. PMID: 37887781 Free PMC article. Review.
-
Metagenomic next-generation sequencing promotes diagnosis and treatment of Pneumocystis jirovecii pneumonia in non-HIV infected children: a retrospective study.BMC Pulm Med. 2024 Jul 12;24(1):338. doi: 10.1186/s12890-024-03135-1. BMC Pulm Med. 2024. PMID: 38997717 Free PMC article.
-
Immune checkpoint inhibitor increased mortality in lung cancer patients with Pneumocystis jirovecii pneumonia: a comparative retrospective cohort study.Front Oncol. 2024 Jul 5;14:1398357. doi: 10.3389/fonc.2024.1398357. eCollection 2024. Front Oncol. 2024. PMID: 39035737 Free PMC article.
-
Relationship between clinical features and droplet digital PCR copy number in non-HIV patients with pneumocystis pneumonia.BMC Infect Dis. 2023 Nov 27;23(1):833. doi: 10.1186/s12879-023-08580-7. BMC Infect Dis. 2023. PMID: 38012564 Free PMC article.
-
Application of metagenomic next-generation sequencing in the diagnosis of pulmonary invasive fungal disease.Front Cell Infect Microbiol. 2022 Sep 27;12:949505. doi: 10.3389/fcimb.2022.949505. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36237437 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials