

Extraction of Electronic Health Record Data using Fast Healthcare Interoperability Resources for Automated Breast Cancer Risk Assessment
- PMID: 35308910
- PMCID: PMC8861753
Extraction of Electronic Health Record Data using Fast Healthcare Interoperability Resources for Automated Breast Cancer Risk Assessment
Abstract
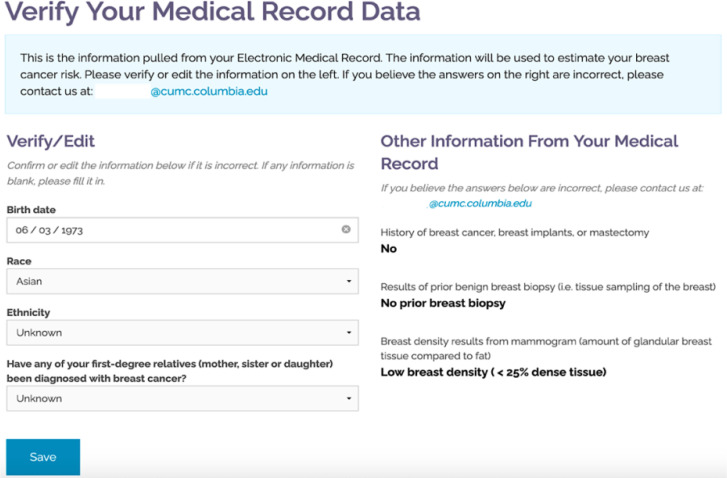
Women at high risk for breast cancer may benefit from enhanced screening and risk-reduction strategies. However, limited time during clinical encounters is one barrier to routine breast cancer risk assessment. We evaluated if electronic health record (EHR) data downloaded using Fast Healthcare Interoperability Resources (FHIR) is sufficient for breast cancer risk calculation in our decision support tools, RealRisks and BNAV. We accessed EHR data using FHIR for six patient advocates, and downloaded and parsed XML documents. We searched for relevant clinical variables, and evaluated if data was sufficient to calculate risk using validated models (Gail, Breast Cancer Screening Consortium [BCSC], BRCAPRO). While only one advocate had sufficient EHR data to calculate risk using the BCSC model only, we identified variables including age, race/ethnicity, mammographic density, and prior breast biopsy in most advocates. EHR data from FHIR could be incorporated into automated breast cancer risk calculation in clinical decision support tools.
©2021 AMIA - All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical