

Using Machine Learning to Support Transfer of Best Practices in Healthcare
- PMID: 35308933
- PMCID: PMC8861698
Using Machine Learning to Support Transfer of Best Practices in Healthcare
Abstract
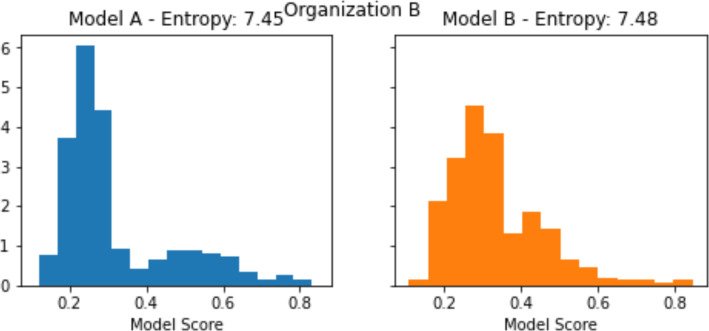
The adoption of best practices has been shown to increase performance in healthcare institutions and is consistently demanded by both patients, payers, and external overseers. Nevertheless, transferring practices between healthcare organizations is a challenging and underexplored task. In this paper, we take a step towards enabling the transfer of best practices by identifying the likely beneficial opportunities for such transfer. Specifically, we analyze the output of machine learning models trained at different organizations with the aims of (i) detecting the opportunity for the transfer of best practices, and (ii) providing a stop-gap solution while the actual transfer process takes place. We show the benefits ofthis methodology on a dataset ofmedical inpatient claims, demonstrating our abilityto identify practice gaps and to support the transfer processes that address these gaps.
©2021 AMIA - All rights reserved.
Figures






References
-
- Berta WB, Baker R. Factors that impact the transfer and retention of best practices for reducing error in hospitals. Health Care Management Review. 2004 Apr 1;29(2):90–7. - PubMed
-
- Tsoukas H, Vladimirou E. What is organizational knowledge? J. Management Studies. 2001 Nov;38(7):973–93.
-
- Guzman G, Fitzgerald JA, Fulop L, Hayes K, Poropat A, Avery M, Campbell S, Fisher R, Gapp R, Herington C, McPhail R. How best practices are copied, transferred, or translated between health care facilities: a conceptual framework. Health Care Management Review. 2015 Jul 1;40(3):193–202. - PubMed
-
- Perleth M, Jakubowski E, Busse R. What is ‘best practice’ in health care? State of the art and perspectives in improving the effectiveness and efficiency of the European health care systems. Health Policy. 2001 Jun 1;56(3):235–50. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous